The average patient intake form takes 8-12 minutes to complete — and another 5-10 minutes of staff time to manually enter into the EHR. Multiply that across 20 patients per day and your front desk is spending two to three hours on data entry that adds zero clinical value. A well-designed patient intake form captures the right information, reduces transcription errors, and gives clinicians what they need before the encounter begins. A poorly designed one wastes everyone's time and introduces compliance risk.
This guide provides eight specialty-specific patient intake form templates — ready to copy, customize, and deploy. Each template covers the fields that matter for that specialty, follows current HIPAA requirements, and can be used as paper forms, digital questionnaires, or converted to conversational AI intake flows. We also cover the compliance checklist every intake form needs, a direct comparison of paper vs. digital vs. AI-powered intake, and how AI is replacing traditional patient intake forms entirely in 2026.
This guide was published in March 2026. Templates and compliance guidance reflect current HIPAA requirements.
What Is a Patient Intake Form?
A patient intake form is a structured document that collects a new or returning patient's demographic, insurance, medical, and consent information before a clinical encounter. It serves three purposes: clinical preparation, legal documentation, and billing verification. Every medical practice — from solo primary care to multi-specialty groups — uses some version of an intake form, whether paper, digital, or increasingly, AI-driven.
Legal foundation. Patient intake forms are not explicitly mandated by HIPAA, but the information they collect is essential for HIPAA compliance. The Privacy Rule requires covered entities to obtain a signed acknowledgment of the Notice of Privacy Practices (NPP) before the first service delivery. The intake form is where this acknowledgment lives. Additionally, state medical practice acts and payer contracts require documented patient consent for treatment and assignment of benefits — both standard intake form components.
Clinical function. A complete intake form gives the clinician a baseline before the encounter starts. Chief complaint, medication list, allergy history, surgical history, and family history — all captured on the intake form — shape the differential diagnosis before the patient enters the exam room. For specialists, intake forms often include condition-specific screening instruments (PHQ-9 for psychiatry, WOMAC for orthopedics, IPSS for urology) that quantify symptom severity and track outcomes over time.
What Every Intake Form Must Include (Checklist)
Regardless of specialty, every patient intake form template should include these ten sections. Missing any of them creates compliance gaps, billing problems, or incomplete clinical records.
- Patient demographics — Full legal name, date of birth, gender, address, phone number, email, preferred language, race/ethnicity (required for federal reporting in many programs)
- Insurance information — Primary and secondary insurance carrier, policy number, group number, policyholder name and relationship, insurance phone number, prior authorization details if applicable
- Medical history — Past diagnoses, chronic conditions, hospitalizations, surgeries, and dates. This is the backbone of clinical decision-making
- Current medications — Drug name, dosage, frequency, prescribing provider. Include over-the-counter medications and supplements
- Allergies — Drug allergies with reaction type (anaphylaxis vs. rash vs. GI upset), food allergies, latex allergy, environmental allergies
- Social history — Tobacco use (pack-years), alcohol use (drinks per week), recreational drug use, occupation, exercise habits, living situation
- Family history — First-degree relatives with chronic conditions: diabetes, heart disease, cancer (type and age at diagnosis), mental health conditions, autoimmune disorders
- Consent for treatment — Written authorization for the provider to examine, diagnose, and treat. Must be signed and dated
- HIPAA acknowledgment — Signed confirmation that the patient received the Notice of Privacy Practices. Required before first service delivery under the Privacy Rule
- Emergency contact — Name, relationship, phone number. Separate from the patient's own contact information
- Reason for visit / chief complaint — In the patient's own words. This drives the encounter and determines medical necessity for billing
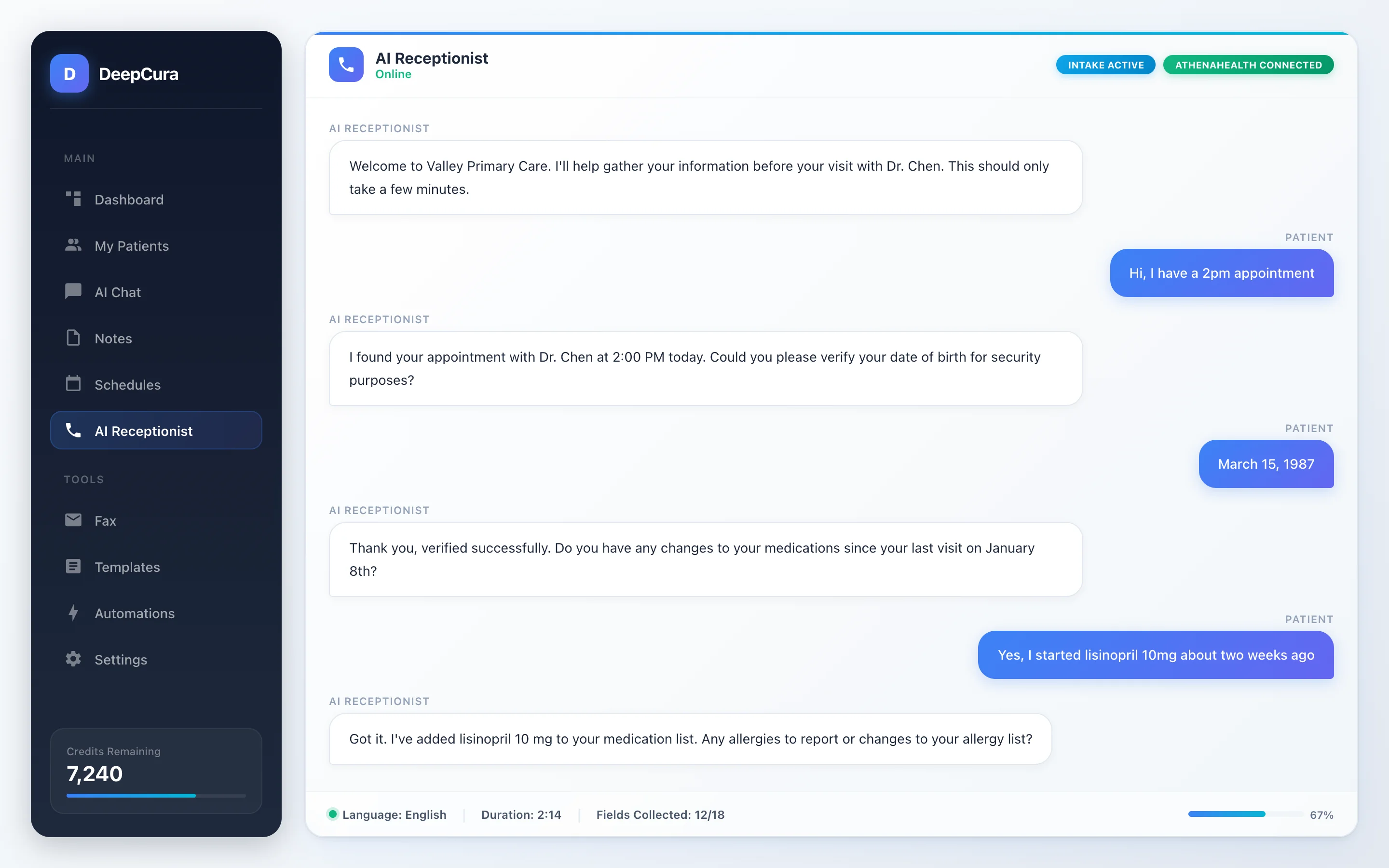 Screenshot: DeepCura AI receptionist — automated patient intake through natural conversation.
Screenshot: DeepCura AI receptionist — automated patient intake through natural conversation.
Skip the Paper Forms — Try AI Intake
DeepCura's AI receptionist handles patient intake automatically. Calls, scheduling, and pre-visit data collection — no forms needed. $129/mo.
+1 (415) 549-1829Available 24/7 · Set up in seconds · No credit card required
Templates by Specialty
The following eight patient intake form templates cover the most commonly needed specialties. Each template is structured as a section-by-section field list that you can directly copy into your practice management system, print as a paper form, or adapt into a digital questionnaire. Fields marked with an asterisk (*) are considered required for complete documentation and billing compliance. If you also need documentation templates for after the encounter, see our doctor's note templates guide.
1. General/Primary Care
Primary care intake forms need to capture the broadest range of information because PCPs serve as the entry point for the entire healthcare system. The form must support preventive care, chronic disease management, acute visits, and referral coordination — all from a single document. A thorough primary care patient intake form template also reduces the burden on the encounter itself, giving the clinician a head start on the history of present illness.
Section A: Patient Demographics
- Full legal name*
- Preferred name (if different)
- Date of birth*
- Gender / Sex assigned at birth*
- Address (street, city, state, ZIP)*
- Phone number (primary and secondary)*
- Email address
- Preferred language*
- Race/Ethnicity
- Marital status
- Emergency contact name, relationship, and phone*
Section B: Insurance Information
- Primary insurance carrier and phone*
- Policy/Member ID*
- Group number
- Policyholder name and relationship to patient*
- Secondary insurance (if applicable)
- Workers' compensation or auto accident (Y/N)
Section C: Medical History
- Current medical conditions / active diagnoses*
- Past medical conditions (resolved)
- Surgical history with dates*
- Hospitalizations with dates and reasons
- History of blood transfusions (Y/N)
Section D: Medications and Allergies
- Current prescription medications (name, dose, frequency)*
- Over-the-counter medications and supplements
- Drug allergies with reaction type*
- Food allergies
- Latex allergy (Y/N)
Section E: Family History
- Heart disease (which relative, age of onset)
- Diabetes (Type 1 or 2, which relative)
- Cancer (type, which relative, age at diagnosis)
- Stroke / hypertension
- Mental health conditions
- Autoimmune disorders
- Other hereditary conditions
Section F: Social History
- Tobacco use (current/former/never, pack-years)*
- Alcohol use (drinks per week)*
- Recreational drug use (current/former/never)*
- Occupation*
- Exercise habits (type, frequency)
- Diet description
- Living situation (alone, with family, assisted living)
- Advance directive on file (Y/N)
Section G: Review of Systems (Abbreviated)
- Constitutional: Fever, weight change, fatigue
- HEENT: Vision changes, hearing loss, sore throat
- Cardiovascular: Chest pain, palpitations, swelling
- Respiratory: Cough, shortness of breath, wheezing
- GI: Nausea, abdominal pain, bowel changes
- Musculoskeletal: Joint pain, stiffness, weakness
- Neurological: Headaches, dizziness, numbness
- Psychiatric: Anxiety, depression, sleep changes
Section H: Reason for Visit
- Chief complaint (in patient's own words)*
- When did symptoms begin?
- What makes it better or worse?
Section I: Consent and Compliance
- Consent for treatment (signature and date)*
- HIPAA Notice of Privacy Practices acknowledgment (signature and date)*
- Assignment of benefits / financial responsibility (signature and date)*
- Release of information authorization (optional)
2. Pediatrics
Pediatric intake forms require information that adult forms do not — guardian details, birth history, developmental milestones, immunization records, and school performance. The legal consent structure is different too: a parent or legal guardian must sign all consent and HIPAA acknowledgment sections. For adolescents, state-specific minor consent laws may allow the patient to consent independently for certain services (reproductive health, substance use, mental health) — your form should accommodate this.
Section A: Patient Demographics
- Child's full legal name*
- Date of birth*
- Gender / Sex assigned at birth*
- Address*
- Parent/Guardian #1: Name, relationship, phone, email*
- Parent/Guardian #2: Name, relationship, phone, email
- Emergency contact (if different from guardians)*
- Custody arrangement (if applicable)
- Preferred language*
- School name and grade level
Section B: Insurance Information
- Primary insurance carrier*
- Policy/Member ID*
- Group number
- Policyholder name and relationship*
- Medicaid/CHIP ID (if applicable)
Section C: Birth and Developmental History
- Birth weight and gestational age*
- Delivery type (vaginal / C-section)*
- Complications during pregnancy or delivery
- NICU stay (Y/N, duration)
- Breastfed / formula fed / combination
- Developmental milestones: First words (age), first steps (age), toilet trained (age)
- Speech or language delays (Y/N)
- Learning disabilities or IEP/504 plan (Y/N)
Section D: Immunization Record
- Immunization history (attach records or provide dates)*
- Any vaccines declined (list and reason)
- Adverse reactions to prior vaccines
Section E: Medical History
- Current medical conditions*
- Past illnesses (chickenpox, ear infections, strep, RSV)
- Surgical history with dates
- Hospitalizations with dates and reasons
- Prior ER visits
Section F: Medications and Allergies
- Current medications (name, dose, frequency)*
- Vitamins or supplements
- Drug allergies with reaction type*
- Food allergies (critical for school forms)
- Environmental allergies
Section G: Family History
- Asthma / allergies
- Diabetes
- Heart disease
- Cancer
- Seizure disorders
- Developmental or genetic conditions
- Mental health conditions (ADHD, autism, anxiety, depression)
Section H: Social History
- Number of siblings
- Who lives in the household*
- Childcare / daycare arrangements
- Pets in the home
- Secondhand smoke exposure (Y/N)*
- Firearms in the home (stored safely Y/N)
- Screen time (hours per day)
Section I: Reason for Visit
- Chief complaint*
- New patient or established patient transfer*
- Records to request from prior pediatrician
Section J: Consent and Compliance
- Parent/Guardian consent for treatment (signature and date)*
- HIPAA acknowledgment (signed by parent/guardian)*
- Authorization to communicate with school nurse (optional)
- Photo/media consent for minors (optional)
3. Psychiatry/Mental Health
Mental health intake forms are the most clinically intensive of any specialty. The intake itself often functions as a mini-assessment — capturing psychiatric history, validated screening scores, substance use patterns, safety risk factors, and trauma exposure. A thorough psychiatry patient intake form template should include embedded screening instruments (PHQ-9 for depression, GAD-7 for anxiety) because these become part of the clinical record and support medical necessity documentation. For a deeper dive on the biopsychosocial assessment framework that underpins psychiatric intake, see our full guide.
Section A: Patient Demographics
- Full legal name*
- Date of birth*
- Gender identity and pronouns
- Address*
- Phone and email*
- Emergency contact*
- Preferred language*
- Referred by (self, PCP, therapist, other)
Section B: Insurance Information
- Primary insurance carrier and phone*
- Policy/Member ID*
- Group number
- Policyholder name and relationship*
- Prior authorization status for behavioral health
Section C: Psychiatric History
- Previous psychiatric diagnoses*
- Current symptoms and duration*
- Prior psychiatric hospitalizations (dates, facilities, reasons)
- Previous suicide attempts (dates, methods, outcomes)*
- History of self-harm (Y/N, method, last occurrence)*
- Prior psychiatric medications (name, dose, duration, reason for discontinuation, effectiveness)*
- Current therapist/counselor (name, frequency, modality)
- Previous therapy types (CBT, DBT, EMDR, psychodynamic, group, other)
- ECT or TMS history (Y/N)
Section D: Validated Screening Instruments
- PHQ-9 (Patient Health Questionnaire — depression severity)*
- GAD-7 (Generalized Anxiety Disorder scale)*
- AUDIT-C (Alcohol Use Disorders Identification Test — brief)
- PCL-5 (PTSD Checklist) — if trauma history indicated
- Columbia Suicide Severity Rating Scale (C-SSRS) — for safety screening*
Section E: Substance Use History
- Alcohol: Current use, frequency, quantity, CAGE/AUDIT score*
- Cannabis: Current use, frequency, method
- Stimulants (cocaine, methamphetamine): Current/former/never
- Opioids (prescription or illicit): Current/former/never
- Benzodiazepines (non-prescribed): Current/former/never
- Tobacco/nicotine: Current/former/never, quantity*
- Other substances
- Prior substance use treatment (detox, rehab, MAT, AA/NA)
- Sobriety date (if in recovery)
Section F: Safety Screening
- Current suicidal ideation (Y/N)*
- Suicidal plan or intent (Y/N)*
- Access to firearms (Y/N)*
- Current homicidal ideation (Y/N)*
- History of violence or aggression
- Current domestic violence (victim or perpetrator)
- Dependent adults or children at risk
Section G: Medical History
- Current medical conditions*
- Thyroid disorders (common psychiatric mimic)
- Traumatic brain injury history
- Seizure disorder
- Chronic pain conditions
- Sleep disorders
- Current non-psychiatric medications*
Section H: Social History
- Living situation*
- Relationship status
- Employment / disability status*
- Education level
- Legal involvement (current charges, probation, custody disputes)
- Military service history
- Trauma history: childhood abuse, neglect, sexual assault, combat, accidents*
- Cultural or religious considerations for treatment
- Social support network
Section I: Reason for Visit
- Chief complaint (in patient's own words)*
- Goals for treatment*
- Preferred treatment approach (medication, therapy, combination)
Section J: Consent and Compliance
- Consent for psychiatric treatment (signature and date)*
- HIPAA acknowledgment*
- Consent for controlled substance prescribing (if applicable)
- Telehealth consent (if applicable)
- 42 CFR Part 2 consent (for substance use disorder records — separate from standard HIPAA)
4. Orthopedics/Sports Medicine
Orthopedic intake centers on the musculoskeletal complaint — mechanism of injury, functional limitations, pain characteristics, and prior interventions. The form needs to capture enough detail for the surgeon or sports medicine physician to determine whether imaging, conservative treatment, or surgical referral is appropriate before the exam begins. Activity level and functional goals are critical because they directly influence treatment decisions — a competitive athlete and a sedentary retiree with the same MRI findings may receive completely different care plans. For a comparison of AI scribes built for orthopedic workflows, see our Best AI Scribe for Orthopedics guide.
Section A: Patient Demographics
- Full legal name*
- Date of birth*
- Gender*
- Address*
- Phone and email*
- Emergency contact*
- Occupation and job physical demands*
- Dominant hand (L/R)*
Section B: Insurance Information
- Primary insurance carrier*
- Policy/Member ID*
- Group number
- Workers' compensation claim (Y/N, claim number, adjuster contact)*
- Auto accident claim (Y/N, date of accident, attorney contact)
- Prior authorization status
Section C: Chief Complaint and Injury Details
- Body part(s) affected*
- Date of onset / date of injury*
- Mechanism of injury (how it happened)*
- Was this a work injury (Y/N)*
- Was this a sports injury (Y/N, sport, level of play)
- Gradual onset vs. acute event*
- Prior treatment for this condition (PT, injections, bracing, surgery)
- Imaging already completed (X-ray, MRI, CT — dates and locations)
Section D: Pain Assessment
- Current pain level (0-10 numeric rating scale)*
- Pain at worst (0-10)*
- Pain at best (0-10)
- Pain character (sharp, dull, aching, burning, throbbing, shooting)*
- Aggravating factors*
- Relieving factors*
- Pain medications currently used (name, dose, effectiveness)
- Pain interference with sleep (Y/N)
Section E: Functional Assessment
- Current activity restrictions*
- Difficulty with: Walking, stairs, sitting, standing, lifting, gripping, reaching
- Assistive devices used (cane, crutch, brace, wheelchair)
- Sports/exercise: Current participation level vs. prior level*
- Work status: Full duty / modified duty / off work*
Section F: Surgical History
- Prior orthopedic surgeries (body part, procedure, date, surgeon)*
- Other surgeries
- Anesthesia complications (Y/N)
- Hardware currently in body (plates, screws, joint replacements)
Section G: Medical History
- Diabetes (affects healing)*
- Osteoporosis / osteopenia
- Rheumatoid arthritis or autoimmune conditions
- Blood clotting disorders or anticoagulant use*
- Cardiac history
- Current medications*
- Drug allergies with reaction type*
Section H: Social History
- Tobacco use (affects bone healing)*
- Alcohol use*
- Recreational drug use
- Exercise history and fitness level*
- Activity goals (return to sport, return to work, pain-free daily living)*
Section I: Consent and Compliance
- Consent for treatment (signature and date)*
- HIPAA acknowledgment*
- Imaging consent (if applicable)
- Workers' comp authorization to release records (if applicable)
5. OB/GYN
OB/GYN intake forms serve dual populations — obstetric patients and gynecologic-only patients — and the form should branch accordingly. Obstetric intake requires a complete pregnancy history (gravida/para, prior complications, delivery methods), while gynecologic intake focuses on menstrual history, contraception, screening history, and sexual health. Both need comprehensive family history because hereditary conditions like BRCA mutations, preeclampsia risk, and gestational diabetes have direct clinical implications.
Section A: Patient Demographics
- Full legal name*
- Date of birth*
- Gender identity*
- Address*
- Phone and email*
- Emergency contact*
- Preferred language*
- Partner/spouse name (optional)
Section B: Insurance Information
- Primary insurance carrier*
- Policy/Member ID*
- Group number
- Policyholder name and relationship*
- Medicaid pregnancy coverage (if applicable)
Section C: Menstrual History
- Age at first period (menarche)*
- Last menstrual period (LMP) — first day*
- Cycle length (days)*
- Cycle regularity (regular / irregular)*
- Duration of period (days)
- Heavy bleeding (menorrhagia) (Y/N)
- Painful periods (dysmenorrhea) (Y/N, severity)
- Intermenstrual bleeding or spotting (Y/N)
- Menopausal status (pre / peri / post)*
Section D: Pregnancy History (Obstetric)
- Gravida (total pregnancies)*
- Para (term births, preterm births, abortions/miscarriages, living children — TPAL)*
- For each prior pregnancy: Year, gestational age at delivery, delivery type, birth weight, complications
- History of: Preeclampsia, gestational diabetes, preterm labor, C-section, postpartum depression
- Currently pregnant (Y/N)*
- Estimated due date (if pregnant)
Section E: Gynecologic History
- Current contraception method*
- Prior contraception methods and reasons for discontinuation
- Last Pap smear (date and result)*
- Last mammogram (date and result, if age-appropriate)*
- History of abnormal Pap results (Y/N, diagnosis, treatment)
- HPV vaccination status
- STI history (chlamydia, gonorrhea, herpes, syphilis, HIV)
- History of: Fibroids, ovarian cysts, endometriosis, PCOS, pelvic inflammatory disease
- Prior gynecologic surgeries (hysterectomy, LEEP, D&C, laparoscopy)
Section F: Sexual Health
- Sexually active (Y/N)*
- Number of current partners
- Partner gender(s)
- Dyspareunia (painful intercourse) (Y/N)
- Fertility concerns (Y/N)
- History of sexual assault or abuse (optional — with trauma-informed framing)
Section G: Medical History and Medications
- Current medical conditions*
- Thyroid disorders
- Blood clotting disorders (especially relevant for contraception decisions)*
- Migraines with aura (contraindication for estrogen-containing contraceptives)*
- Current medications*
- Drug allergies with reaction type*
- Supplements (folic acid, prenatal vitamins)
Section H: Family History
- Breast cancer (which relative, age at diagnosis, BRCA status)*
- Ovarian cancer*
- Cervical cancer
- Preeclampsia in mother or sisters
- Gestational diabetes in mother or sisters
- Blood clotting disorders (Factor V Leiden, etc.)
- Birth defects or genetic conditions
Section I: Social History
- Tobacco use*
- Alcohol use*
- Recreational drug use*
- Domestic violence screening (HITS or similar tool)*
- Occupation
- Exercise habits
Section J: Reason for Visit
- Chief complaint / reason for visit*
- Annual exam / new OB / problem visit / follow-up*
- Specific concerns or questions for the provider
Section K: Consent and Compliance
- Consent for treatment (signature and date)*
- HIPAA acknowledgment*
- Consent for pelvic examination (separate consent recommended)*
- Pregnancy testing consent (if applicable)
6. Dermatology
Dermatology intake is visually oriented — the form needs to capture where the lesion is, how long it has been there, how it has changed, and what the patient has already tried. Sun exposure history and family skin cancer history are critical screening elements that primary care forms rarely cover in sufficient detail. A good dermatology patient intake form template includes a body diagram for the patient to mark the location of concern, though in a text-based format, anatomical description fields serve the same purpose.
Section A: Patient Demographics
- Full legal name*
- Date of birth*
- Gender*
- Address*
- Phone and email*
- Emergency contact*
- Referring provider (if applicable)
- Skin type (Fitzpatrick scale I-VI, if known)
Section B: Insurance Information
- Primary insurance carrier*
- Policy/Member ID*
- Group number
- Policyholder name and relationship*
- Prior authorization status (for procedures/biologics)
Section C: Chief Complaint — Skin Concern
- Location(s) on body*
- Duration (when first noticed)*
- Size change: Growing / stable / shrinking*
- Color change (Y/N, describe)*
- Symptoms: Itching, burning, pain, bleeding, oozing*
- Triggers or aggravating factors (sun, heat, stress, products)
- Similar lesions in the past (Y/N)
- Cosmetic concern vs. medical concern*
Section D: Treatment History for Current Concern
- Over-the-counter treatments tried (products, duration, effectiveness)
- Prescription topicals tried (name, duration, effectiveness)
- Oral medications tried for skin condition
- Prior procedures (biopsy, excision, cryotherapy, laser)
- Biopsy results (if known)
Section E: Dermatologic History
- History of skin cancer (type, location, treatment, year)*
- History of: Eczema, psoriasis, acne, rosacea, vitiligo, alopecia
- History of abnormal moles or dysplastic nevi
- Prior dermatologic procedures (Mohs surgery, chemical peels, laser resurfacing)
- Current skincare routine (cleanser, moisturizer, sunscreen, retinoids)
Section F: Sun Exposure and Risk Factors
- Tanning bed use (current/former/never)*
- History of blistering sunburns (number, approximate ages)*
- Daily sun exposure (hours/day, occupational vs. recreational)*
- Sunscreen use (frequency: daily / sometimes / rarely / never)*
- Outdoor occupation (Y/N)
Section G: Family History
- Melanoma (which relative)*
- Other skin cancers (basal cell, squamous cell)
- Psoriasis
- Eczema / atopic dermatitis
- Autoimmune conditions (lupus, dermatomyositis)
Section H: Medical History and Medications
- Current medical conditions*
- Autoimmune conditions (relevant for biologic eligibility)
- Immunosuppression or HIV status (affects skin pathology)*
- Current medications* (including those causing photosensitivity)
- Drug allergies with reaction type*
- Latex allergy (Y/N — important for exam gloves and procedures)
Section I: Social History
- Tobacco use*
- Alcohol use
- Occupation*
- Hobbies with skin exposure risk (gardening, welding, swimming)
Section J: Consent and Compliance
- Consent for treatment (signature and date)*
- HIPAA acknowledgment*
- Consent for clinical photography (separate consent)*
- Consent for biopsy/procedure (if applicable)
7. Cardiology
Cardiology intake forms prioritize cardiac-specific risk factors, functional capacity, and medication reconciliation — particularly anticoagulants, antihypertensives, and lipid-lowering drugs. The form should capture exercise tolerance in concrete terms (blocks walked, flights of stairs, NYHA functional class) because this directly informs diagnostic workup and treatment intensity. Family cardiac history is weighted more heavily in cardiology than in any other specialty — a first-degree relative with premature coronary artery disease fundamentally changes risk stratification.
Section A: Patient Demographics
- Full legal name*
- Date of birth*
- Gender*
- Address*
- Phone and email*
- Emergency contact*
- Referring provider*
- Height and weight (for BMI and drug dosing)*
Section B: Insurance Information
- Primary insurance carrier*
- Policy/Member ID*
- Group number
- Policyholder name and relationship*
- Prior authorization status (for imaging, procedures, devices)
Section C: Cardiac History
- Known cardiac diagnoses* (coronary artery disease, heart failure, atrial fibrillation, valvular disease, cardiomyopathy, congenital heart disease)
- Prior cardiac events: Heart attack (date, treatment), stroke/TIA (date), cardiac arrest
- Prior cardiac procedures*: Catheterization (date, findings), stent placement (number, locations, dates), CABG (date, grafts), valve repair/replacement, pacemaker/ICD implant (date, manufacturer, model)
- Prior cardiac imaging: Echocardiogram (date, EF%), stress test (date, result), cardiac CT/MRI
- Known ejection fraction (EF%) if available
Section D: Current Symptoms
- Chest pain or pressure (Y/N, character, triggers, frequency)*
- Shortness of breath at rest (Y/N)*
- Shortness of breath with exertion (Y/N, at what level of activity)*
- Orthopnea (how many pillows to sleep)*
- Paroxysmal nocturnal dyspnea (Y/N)
- Palpitations (Y/N, regular or irregular, duration)*
- Syncope or presyncope (Y/N, circumstances)*
- Lower extremity edema (Y/N)*
- Claudication (leg pain with walking) (Y/N)
- NYHA Functional Class (I-IV)*
Section E: Cardiac Risk Factors
- Hypertension (Y/N, years, current treatment)*
- Diabetes (Y/N, Type 1/2, HbA1c if known)*
- Hyperlipidemia (Y/N, last lipid panel results)*
- Obesity (BMI > 30)*
- Tobacco use (current/former/never, pack-years)*
- Family history of premature CAD (male relative < 55, female relative < 65)*
- Sedentary lifestyle (Y/N)
- Obstructive sleep apnea (Y/N, on CPAP)*
- Chronic kidney disease (Y/N, stage)
Section F: Exercise Tolerance
- Current exercise: Type, frequency, duration*
- Blocks walked without stopping*
- Flights of stairs without stopping*
- Limitations: Chest pain, shortness of breath, fatigue, leg pain
- Participation in cardiac rehabilitation (current/prior/never)
Section G: Medications (Comprehensive Reconciliation)
- Anticoagulants/Antiplatelets: Warfarin (INR range), DOACs, aspirin, clopidogrel*
- Antihypertensives: Beta-blockers, ACE inhibitors/ARBs, calcium channel blockers, diuretics*
- Lipid-lowering: Statins (name, dose), ezetimibe, PCSK9 inhibitors*
- Antiarrhythmics: Amiodarone, flecainide, sotalol, dofetilide
- Heart failure meds: SGLT2 inhibitors, sacubitril/valsartan, hydralazine/nitrate
- Nitrates: Nitroglycerin (SL or patch)
- All other current medications
- Drug allergies with reaction type*
Section H: Family Cardiac History
- Heart attack (which relative, age at event)*
- Sudden cardiac death (which relative, age)*
- Heart failure
- Atrial fibrillation
- Cardiomyopathy (hypertrophic, dilated)
- Aortic aneurysm
- Congenital heart disease
Section I: Social History
- Tobacco use (detailed: pack-years, quit date)*
- Alcohol use (drinks per week)*
- Caffeine intake
- Recreational drug use (cocaine is specifically cardiotoxic)*
- Occupation and physical demands
- Stress level and coping
Section J: Reason for Visit
- Chief complaint*
- New patient vs. follow-up vs. second opinion*
- Specific questions or concerns for the cardiologist
Section K: Consent and Compliance
- Consent for treatment (signature and date)*
- HIPAA acknowledgment*
- Consent for stress testing (if applicable)
- Consent to receive results by patient portal/phone
8. Urgent Care/Walk-In
Urgent care intake must be fast. Patients arrive unscheduled with acute complaints — the form needs to capture enough information for safe triage and treatment without the depth of a primary care new patient intake. Chief complaint, acuity level, medication list, and allergies are the critical elements. The form should also capture PCP and pharmacy information because urgent care is episodic — the PCP needs a visit summary, and prescriptions need a destination. Keep the form to two pages maximum. Patients with lacerations and 102-degree fevers do not have patience for a five-page questionnaire.
Section A: Patient Demographics
- Full legal name*
- Date of birth*
- Gender*
- Address*
- Phone*
- Emergency contact*
- Primary care provider (name, practice, phone)*
- Preferred pharmacy (name, address, phone)*
Section B: Insurance Information
- Primary insurance carrier*
- Policy/Member ID*
- Group number
- Policyholder name and relationship*
- Photo ID presented (Y/N)*
Section C: Chief Complaint and Triage
- Reason for visit (in patient's own words)*
- When did symptoms start?*
- Severity (1-10)*
- Is this a work injury? (Y/N)*
- Is this related to an accident? (Y/N, type)*
- Have you been seen elsewhere for this issue? (Y/N, where, when)
- Fever (Y/N, temperature if known)*
- Recent travel (Y/N, where)
- COVID/flu/strep exposure (Y/N)
Section D: Medical History (Brief)
- Major medical conditions*
- Prior surgeries*
- Current medications (name, dose)*
- Drug allergies with reaction type*
- Last tetanus shot (date, if known — critical for wound care)
Section E: Women's Health (If Applicable)
- Currently pregnant (Y/N)*
- Last menstrual period*
- Breastfeeding (Y/N)
Section F: Social History (Brief)
- Tobacco use (Y/N)*
- Alcohol use (Y/N)
- Recreational drug use (Y/N)
Section G: Consent and Compliance
- Consent for treatment (signature and date)*
- HIPAA acknowledgment*
- Financial responsibility acknowledgment*
- Consent to send visit summary to PCP (Y/N)*
Paper vs. Digital vs. AI Intake
Most practices are still deciding between paper and digital intake forms. A growing minority — particularly tech-forward and multi-location groups — are skipping digital forms entirely and moving to AI-powered conversational intake. Here is how the three approaches compare across the metrics that matter most to practice operations.
| Feature | Paper Forms | Digital Forms | AI-Powered Intake |
|---|---|---|---|
| Setup Cost | Low | Medium | Medium |
| Patient Experience | Poor (clipboard, pen) | Better (tablet/phone) | Best (conversational) |
| Data Entry Errors | High (handwriting) | Medium (typos) | Low (structured AI) |
| Staff Time | High (manual entry) | Medium (some automation) | Minimal |
| HIPAA Compliance | Difficult (physical storage) | Good (with encryption) | Best (automated audit) |
| EHR Integration | None (manual entry) | Partial | Full |
| Multilingual Support | Expensive (printed translations) | Good | Best (real-time translation) |
| Update Frequency | Expensive (reprint) | Easy | Automatic |
| Completion Rate | 60-70% (patients skip fields) | 75-85% | 90%+ (AI prompts for missing data) |
| Average Completion Time | 12-15 minutes | 8-10 minutes | 5-7 minutes (conversational) |
Paper forms still dominate in practices with older patient populations, limited IT resources, or low visit volumes where the cost of digitization exceeds the labor savings. The primary liability is data entry — someone on staff must read handwriting, interpret abbreviations, and type everything into the EHR. Error rates on manual transcription range from 2-5%, and those errors propagate into billing, medication lists, and clinical decision-making.
Digital forms — delivered via tablet in the waiting room, patient portal link, or pre-visit email — eliminate the handwriting problem and can enforce required fields. Most practice management systems (athenahealth, eClinicalWorks, Epic) offer built-in digital intake, though the forms are often rigid, poorly designed, and frustrating for patients. Third-party solutions like Phreesia and Intakeq provide better UX but add another vendor and another monthly cost.
AI-powered intake represents the next evolution. Instead of handing patients a form — paper or digital — an AI system collects the same information through a natural conversation, either by phone call before the visit or via a chat interface. The AI asks follow-up questions, handles branching logic automatically (skipping pregnancy questions for male patients, for example), and pushes structured data directly into the EHR. For practices using DeepCura's AI receptionist, the intake happens during the scheduling call itself — one touchpoint instead of two.
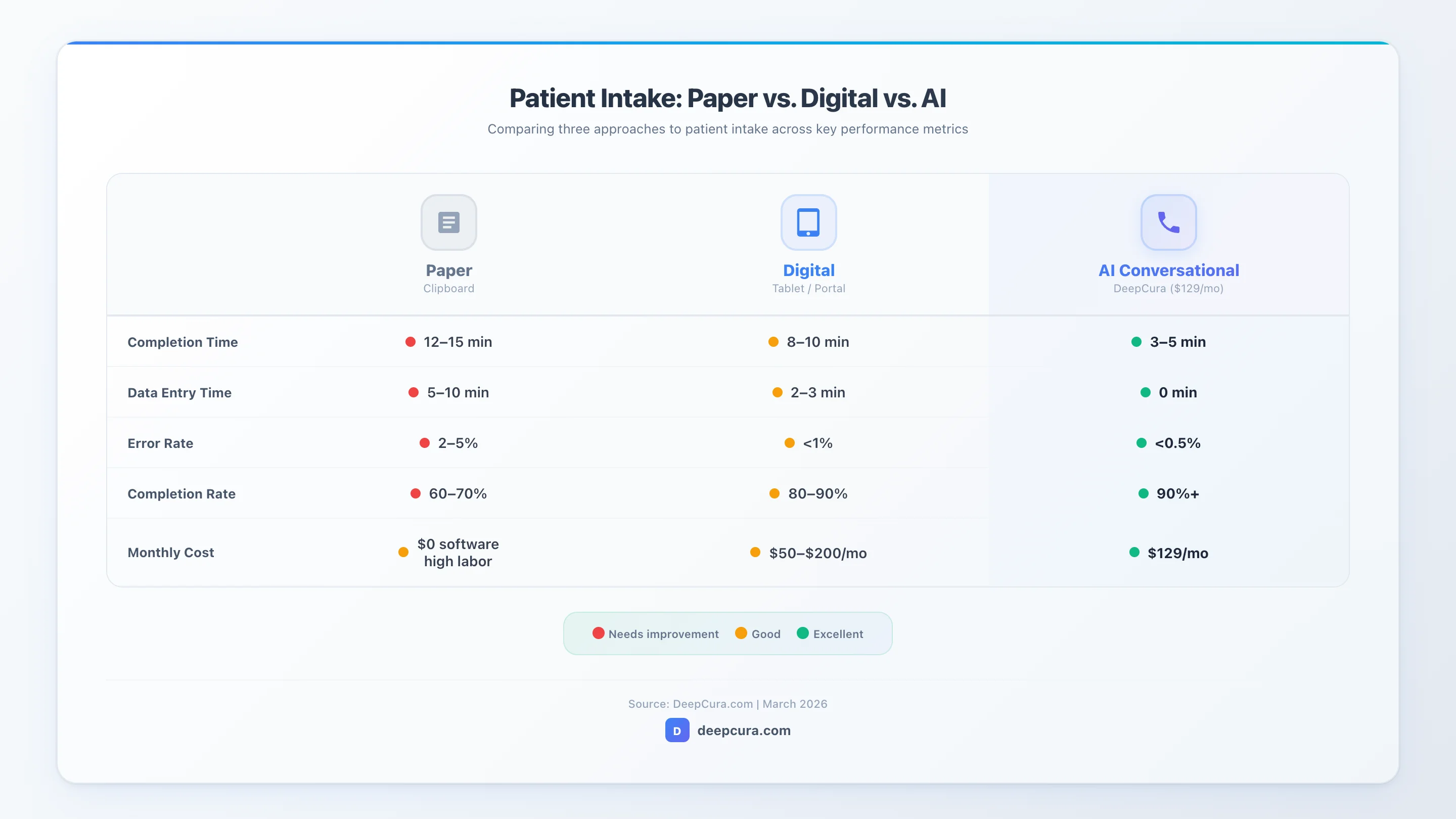 Infographic: Paper vs. digital vs. AI intake — comparing completion time, error rates, and cost per patient.
Infographic: Paper vs. digital vs. AI intake — comparing completion time, error rates, and cost per patient.
Automate Patient Intake with AI
DeepCura's AI receptionist collects patient information via phone calls, handles scheduling, and pushes data to your EHR — before the patient walks in.
+1 (415) 549-1829Available 24/7 · Set up in seconds · No credit card required
How AI Is Replacing Patient Intake Forms in 2026
The patient intake form has not fundamentally changed in 40 years. The format shifted from paper to PDF to tablet, but the experience remained the same — a long list of fields that patients fill out in silence, often incompletely, and staff re-enter manually. In 2026, AI-powered intake is breaking that pattern by replacing forms with conversations.
How it works. An AI system — typically a voice agent or chat assistant — contacts the patient before their appointment (or handles their inbound scheduling call) and collects intake information through natural dialogue. The patient says "I take metformin 500 twice a day and lisinopril 10 once a day" instead of writing it in a tiny box. The AI parses the response into structured medication data — drug name, dosage, frequency — and pushes it directly to the EHR. No clipboard. No data entry. No handwriting interpretation.
The clinical advantage is completeness. Paper and digital forms rely on the patient to understand and correctly answer medical questions. Patients routinely skip fields they do not understand, abbreviate medication names incorrectly, or leave allergy sections blank because they "can't remember." AI intake systems ask follow-up questions — "You mentioned you're allergic to penicillin. Do you know what kind of reaction you had? Was it a rash, difficulty breathing, or something else?" — that improve data quality in ways static forms cannot.
DeepCura's AI receptionist is purpose-built for this. When a patient calls to schedule an appointment — or when the practice initiates a pre-visit outbound call — DeepCura's voice agent handles scheduling and intake in a single conversation. It verifies identity, collects demographics, confirms insurance, reviews medications and allergies, documents the chief complaint, and pushes everything to the EHR before the patient arrives. The entire interaction takes three to five minutes. It supports 34 languages, runs 24/7, and maintains full HIPAA compliance with a signed BAA and encrypted data handling.
This is the capability gap that separates full-stack clinical AI platforms from scribe-only tools. Products like Freed AI and other AI medical scribes focus exclusively on in-encounter documentation — they record the visit and generate a note. That is valuable, but it does nothing for the pre-visit workflow. DeepCura automates the entire patient journey: first phone call, scheduling, intake data collection, in-encounter ambient scribing, ICD-10 and CPT coding, and billing. Intake is not a standalone feature — it is integrated into the same platform that handles every other clinical AI task.
Key capabilities of AI-powered intake:
- Pre-visit phone calls to collect patient information conversationally
- Inbound call handling for scheduling and triage
- Automatic data structuring and EHR push
- Multilingual support (34 languages with DeepCura)
- 24/7 availability — no staffing required
- HIPAA-compliant with encrypted data handling
- Branching logic that adapts questions based on patient responses
- Follow-up prompts for incomplete or ambiguous answers
- Integration with existing practice management workflows
For practices still distributing paper or digital intake forms, the ROI calculation is straightforward: if your front desk spends two hours per day on intake data entry at $20/hour, that is $10,400 per year in labor costs — plus the downstream cost of data entry errors in billing and clinical records. AI intake at $129/month ($1,548/year) replaces that labor, improves data quality, and gives clinicians a complete chart before the patient walks in.

HIPAA Compliance for Intake Forms
Every patient intake form — paper, digital, or AI-driven — collects protected health information (PHI) and falls under HIPAA regulation. Compliance is not optional, and the penalties for violations are severe: $141 to $71,162 per violation for unknowing breaches (adjusted annually for inflation), up to $2.13 million per year for willful neglect. Understanding what HIPAA requires for intake forms protects your practice and your patients.
The Privacy Rule and minimum necessary standard. HIPAA's Privacy Rule (45 CFR 164.502) requires covered entities to limit PHI collection, use, and disclosure to the minimum necessary for the intended purpose. For intake forms, this means asking only for information that is clinically relevant, operationally necessary, or legally required. A dermatology practice does not need a detailed obstetric history. An urgent care center does not need a three-generation family pedigree. Collect what you need for the specialty and the visit type — nothing more.
Notice of Privacy Practices (NPP). Under 45 CFR 164.520, covered entities must provide patients with a Notice of Privacy Practices that explains how their PHI will be used and disclosed. The patient must acknowledge receipt of the NPP, and this acknowledgment should be documented on the intake form. If the patient refuses to sign, document the refusal and the date — you are not required to refuse treatment, but you must document the attempt.
Patient consent and authorization. Consent for treatment and HIPAA acknowledgment are separate legal instruments, though they often appear on the same intake form. Consent for treatment authorizes the provider to examine and treat the patient. HIPAA acknowledgment confirms the patient received the privacy notice. Some states require additional consent for specific services — HIV testing, genetic testing, substance use disorder treatment (also governed by 42 CFR Part 2), and psychotherapy. Your intake form should include the consent elements required by your state and specialty.
Digital and AI intake compliance. Digital intake forms must be transmitted and stored using encryption that meets HIPAA technical safeguard requirements (45 CFR 164.312). This means encryption in transit (TLS 1.2 or higher) and encryption at rest (AES-256). Patient portals, tablet-based forms, and AI intake systems must all meet these standards. AI-powered intake systems like DeepCura add an additional compliance layer — automated audit trails that log every data access, modification, and transmission. This makes breach investigation faster and simpler than tracking down paper form access logs.
Breach notification. If PHI collected on intake forms is compromised — a stolen laptop with unencrypted digital forms, a misdirected fax, or a breach of a cloud-based intake system — the Breach Notification Rule (45 CFR 164.400-414) requires notification to affected individuals within 60 days, notification to HHS, and, for breaches affecting 500+ individuals, notification to local media. The best protection is prevention: encrypt everything, limit access, use audit trails, and choose vendors with signed Business Associate Agreements (BAAs).
Practical compliance checklist for intake forms:
- Collect only minimum necessary PHI for the visit type
- Include NPP acknowledgment with signature line
- Separate consent for treatment from HIPAA acknowledgment
- Encrypt digital forms in transit and at rest
- Require signed BAA from any third-party intake vendor
- Maintain audit trails for all PHI access
- Train staff on PHI handling during intake
- Store paper forms in locked, access-controlled areas
- Implement automatic session timeout for tablet-based intake
- Document retention policy aligned with state medical records laws
Frequently Asked Questions
What is a patient intake form?
A patient intake form is a document — paper, digital, or AI-collected — that gathers a patient's demographic, insurance, medical history, and consent information before a clinical encounter. It serves as the foundation for the patient's medical record and supports clinical decision-making, billing, and legal compliance.
What should a patient intake form include?
Every patient intake form should include patient demographics, insurance information, medical history, current medications, allergies, family history, social history, consent for treatment, HIPAA acknowledgment, emergency contact information, and the reason for visit. Specialty-specific forms add condition-relevant sections — screening instruments for psychiatry, injury details for orthopedics, menstrual and pregnancy history for OB/GYN.
Are patient intake forms required by HIPAA?
HIPAA does not explicitly mandate a specific intake form. However, HIPAA does require a signed acknowledgment of the Notice of Privacy Practices before the first service delivery, and this acknowledgment is universally captured on the intake form. Additionally, the information collected on intake forms — insurance details, medical history, consent — is required by payer contracts, state medical practice acts, and standard-of-care documentation requirements.
Can I use a free patient intake form template?
Yes. The templates in this guide are free to use and adapt for your practice. The key is customization — a generic template needs to be tailored to your specialty, state-specific consent requirements, and practice workflow. Remove fields that are not relevant to your specialty (minimum necessary standard) and add any screening instruments or consent elements your practice requires. Have your compliance officer or healthcare attorney review the final form before deployment.
What is the best digital patient intake solution?
The best approach depends on your practice size and workflow goals. Traditional digital intake solutions like Phreesia and Intakeq digitize the form experience but still require patients to fill out fields manually. AI-powered intake — like DeepCura's AI receptionist — replaces forms entirely with conversational data collection that pushes structured data directly to the EHR. At $129/month, DeepCura bundles AI intake with ambient scribing, clinical notes, EHR integration, and billing automation.
How do I make my intake forms HIPAA compliant?
Start with the minimum necessary standard — only collect PHI that is required for the visit type. Include a Notice of Privacy Practices acknowledgment with a signature line. For digital forms, ensure encryption in transit (TLS 1.2+) and at rest (AES-256). Require a signed Business Associate Agreement from any third-party vendor that handles intake data. Train staff on PHI handling during the intake process. Store paper forms in locked, access-controlled areas. Maintain audit trails for digital forms. Implement a document retention policy aligned with your state's medical records retention laws.
Can AI replace patient intake forms?
Yes — and it is already happening. AI-powered intake systems collect the same information that traditional forms capture, but through natural conversation instead of static fields. The patient talks to an AI voice agent or chat assistant that asks questions, handles follow-ups, and pushes structured data to the EHR. DeepCura's AI receptionist handles intake during scheduling calls, supporting 34 languages and running 24/7. Completion rates are higher (90%+ vs. 60-70% for paper), data quality improves due to follow-up prompting, and staff time for data entry drops to near zero.
How long should a patient intake form be?
For primary care and specialist new patient visits, intake forms typically run three to five pages. For urgent care, keep it to one to two pages — acuity demands speed. The goal is capturing enough information for safe, informed clinical care without creating a burden that drives incomplete responses. If completion rates are low, the form is too long. AI-powered intake sidesteps this problem entirely — the "form" is a conversation that adapts in length based on the patient's complexity.
Try DeepCura Free — No Credit Card Required
AI receptionist + ambient scribe + EHR integration + billing automation. One platform, $129/mo. Join 6,400+ providers.
+1 (415) 549-1829Available 24/7 · Set up in seconds · No credit card required
For more clinical documentation templates, see our comprehensive SOAP note template guide with 10 free templates across specialties and our doctor's note template for work absence documentation.
References
-
U.S. Department of Health and Human Services. "HIPAA Privacy Rule and Sharing Information Related to Mental Health." HHS.gov. https://www.hhs.gov/hipaa/for-professionals/privacy/index.html
-
Office of the National Coordinator for Health IT. "Health IT Playbook: Privacy and Security." HealthIT.gov. https://www.healthit.gov/playbook/privacy-and-security/
-
American Medical Association. "Documentation and Coding: Best Practices for Medical Records." AMA-assn.org. https://www.ama-assn.org/practice-management/cpt/documentation-and-coding
-
Centers for Medicare & Medicaid Services. "HIPAA Administrative Simplification Statute and Rules." CMS.gov. https://www.cms.gov/Regulations-and-Guidance/Administrative-Simplification/HIPAA-ACA
-
DeepCura. "AI Medical Scribe and Receptionist Platform." DeepCura.com. https://www.deepcura.com
-
Kroenke K, Spitzer RL, Williams JB. "The PHQ-9: Validity of a brief depression severity measure." Journal of General Internal Medicine. 2001;16(9):606-613.
-
Office for Civil Rights. "Breach Notification Rule." HHS.gov. https://www.hhs.gov/hipaa/for-professionals/breach-notification/index.html