10 free templates. 6 real-world examples. One AI shortcut that writes them for you. Studies show clinicians spend an estimated 10-15 minutes per SOAP note — multiply that by 20 patients and you lose over 3 hours a day to documentation alone.
This guide gives you everything you need to cut that to near zero:
- Copy-paste SOAP note templates for primary care, mental health, physical therapy, pediatrics, dermatology, orthopedics, emergency medicine, neurology, cardiology, and chiropractic
- Filled-out SOAP note examples across 6 specialties so you can see exactly what good documentation looks like
- Step-by-step writing guide covering every section — Subjective, Objective, Assessment, and Plan
- AI SOAP note generator breakdown — how ambient AI scribes like DeepCura listen to the encounter and generate a complete, structured SOAP note in seconds
Whether you are a physician, nurse practitioner, therapist, or medical student, the templates below are ready to use today. Or skip templates entirely and let AI write the note while you focus on the patient.
This guide is designed for licensed healthcare professionals — physicians (MD/DO), nurse practitioners (NPs), physician assistants (PAs), therapists, physical therapists, and clinical students. All templates follow standard documentation requirements and can be adapted to your EHR system. They are not intended for patient self-use.
What Is a SOAP Note?
A SOAP note is the most widely used clinical documentation format in healthcare. SOAP stands for Subjective, Objective, Assessment, and Plan — four sections that together create a structured, logical record of every patient encounter.
Developed by Dr. Lawrence Weed in the 1960s as part of the problem-oriented medical record (POMR), the SOAP note format was designed to standardize how clinicians document patient visits. Before SOAP, clinical notes were narrative and unstructured, making it difficult to track patient progress or communicate between providers.
Who uses SOAP notes? Virtually every clinical discipline:
- Physicians (MD/DO) — primary care, internal medicine, all specialties
- Nurse practitioners and physician assistants
- Therapists — psychologists, LCSWs, LPCs, MFTs
- Physical therapists and occupational therapists
- Chiropractors and dentists
- Medical students and residents during clinical rotations
Why SOAP notes matter. Beyond legal documentation requirements, SOAP notes serve three critical functions: (1) continuity of care — any provider can pick up where the last one left off, (2) billing and reimbursement — payers require structured documentation to justify claims, and (3) legal protection — a well-written SOAP note is your best defense in a malpractice or audit scenario. For more on clinical documentation tools, see our guide to the Best AI Medical Scribes in 2026.
SOAP Note Format — The Four Sections Explained
Every SOAP note follows the same four-section structure. Understanding what belongs in each section is the difference between a note that supports your clinical decision-making and one that creates audit risk.
S — Subjective
The Subjective section captures what the patient tells you. This is the patient's perspective on their condition in their own words.
What to include:
- Chief complaint (CC) — the primary reason for the visit in the patient's words (e.g., "I've had a headache for three days")
- History of present illness (HPI) — onset, location, duration, character, aggravating/alleviating factors, radiation, timing, and severity (use the OLDCARTS or OPQRST mnemonic)
- Review of systems (ROS) — relevant positive and negative findings from the patient's self-report
- Past medical history (PMH) — chronic conditions, surgeries, hospitalizations
- Medications — current medications, dosages, and compliance
- Allergies — drug allergies with reaction type
- Family history (FHx) — relevant hereditary conditions
- Social history (SHx) — tobacco, alcohol, drug use, occupation, living situation
- Patient-reported functional status — how symptoms affect daily activities
Use direct patient quotes in the Subjective section when they capture important clinical details. "The pain wakes me up at 3 AM every night" is more clinically specific than "Patient reports nighttime pain." Quoting the patient also strengthens the note's legal defensibility.
O — Objective
The Objective section documents what you observe, measure, and test. This is clinician-generated data — the findings from your physical examination and diagnostic results.
What to include:
- Vital signs — BP, HR, RR, Temp, SpO2, weight, BMI
- Physical examination findings — organized by system (HEENT, cardiovascular, respiratory, musculoskeletal, neurological, skin, etc.)
- Diagnostic results — lab values, imaging reports, ECG findings, pulmonary function tests
- Screening tool scores — PHQ-9, GAD-7, MMSE, VAS pain scale, Oswestry Disability Index
- Functional observations — gait, range of motion, strength testing results
Key rule: The Objective section should contain only measurable, reproducible data. Clinical impressions and interpretations belong in the Assessment section.
A — Assessment
The Assessment section is your clinical analysis. This is where you synthesize the Subjective and Objective data into a diagnosis or differential diagnosis.
What to include:
- Primary diagnosis — the most likely condition, with ICD-10 code
- Differential diagnoses — alternative conditions you considered and why you ruled them in or out
- Clinical reasoning — how the S and O data support your diagnostic conclusion
- Disease progression — for established patients, whether the condition is improving, stable, or worsening
- Complications or risk factors — any identified risks that influence management
The Assessment section is the most important for billing. Payers and auditors evaluate whether the diagnosis is supported by the documented Subjective and Objective findings. If the Assessment does not logically follow from the data, the claim is vulnerable to denial. For ICD-10 coding guidance, see our medical codes reference.
P — Plan
The Plan section documents your clinical decisions and next steps. It should be specific enough that any covering provider could execute the plan without additional clarification.
What to include:
- Medications — new prescriptions, dose changes, refills, discontinuations (include drug name, dose, route, frequency, and duration)
- Procedures — any performed or ordered (with CPT codes where applicable)
- Referrals — specialist referrals with clinical indication
- Diagnostics ordered — labs, imaging, pathology with clinical justification
- Patient education — topics discussed (diet, exercise, smoking cessation, medication adherence)
- Follow-up — return visit timing and criteria for earlier return
- Safety netting — instructions for when to seek urgent/emergent care
Billing compliance. The Plan section directly supports the E/M (Evaluation and Management) coding level. A detailed plan with multiple treatment modalities, ordered diagnostics, and coordinated referrals supports higher complexity coding. A vague plan like "Continue current medications, follow up PRN" may not support the code billed. Always document the medical decision-making that justifies your management choices.
SOAP Note Templates by Specialty
The following 10 templates cover the most common specialties. Each includes the complete S-O-A-P structure with placeholder fields in brackets. Copy the template into your EHR or documentation system and replace the bracketed fields with patient-specific information.
1. Primary Care / Internal Medicine SOAP Note Template
SUBJECTIVE:
CC: "[Chief complaint in patient's words]"
HPI: [Age]-year-old [sex] presents with [symptom] for [duration].
Onset: [sudden/gradual]. Location: [area]. Character: [sharp/dull/
aching/burning]. Severity: [X/10]. Aggravating factors: [list].
Alleviating factors: [list]. Associated symptoms: [list].
ROS: [Pertinent positives and negatives by system]
PMH: [Chronic conditions, surgeries]
Medications: [Current medications with doses]
Allergies: [Drug allergies with reaction type]
SHx: [Tobacco/alcohol/drug use, occupation, exercise]
FHx: [Relevant family history]
OBJECTIVE:
Vitals: BP [X/X], HR [X], RR [X], Temp [X°F], SpO2 [X%],
Weight [X lbs], BMI [X]
General: [Alert, oriented, no acute distress / appearance]
HEENT: [Head, eyes, ears, nose, throat findings]
Neck: [Supple, no lymphadenopathy, thyroid normal]
Cardiovascular: [RRR, no murmurs/gallops/rubs]
Respiratory: [CTA bilaterally, no wheezes/crackles]
Abdomen: [Soft, non-tender, non-distended, normoactive BS]
Musculoskeletal: [ROM, strength, tenderness findings]
Neurological: [CN II-XII intact, sensation, reflexes]
Skin: [Color, turgor, lesions]
Labs/Imaging: [Results if available]
ASSESSMENT:
1. [Primary diagnosis] — [ICD-10 code]
[Clinical reasoning: how S and O findings support this diagnosis]
2. [Secondary diagnosis if applicable] — [ICD-10 code]
3. [Chronic condition management] — [stable/worsening/improved]
PLAN:
1. [Medication: drug, dose, route, frequency, duration]
2. [Diagnostic orders: labs, imaging with clinical indication]
3. [Referrals: specialist, reason]
4. [Patient education: topics discussed]
5. [Follow-up: timing and criteria for earlier return]
6. [Safety netting: when to seek urgent/emergent care]
2. Mental Health / Therapy SOAP Note Template
SUBJECTIVE:
CC: "[Reason for visit in patient's words]"
HPI: [Age]-year-old [sex] presents for [initial evaluation/follow-up/
therapy session #X]. Patient reports [current mood, sleep, appetite,
energy level, concentration]. [Stressors identified]. [Changes since
last session]. [Medication compliance if applicable].
Suicidal ideation: [Denied / Present — if present, document plan,
intent, means, access, and protective factors]
Homicidal ideation: [Denied / Present]
Substance use: [Current patterns — type, frequency, last use]
Functional status: [Work/school/relationship functioning]
OBJECTIVE:
Appearance: [Grooming, dress, hygiene, psychomotor activity]
Behavior: [Cooperative, guarded, agitated, calm]
Speech: [Rate, rhythm, volume, tone]
Mood: "[Patient's stated mood in their words]"
Affect: [Observed — congruent/incongruent, range, intensity]
Thought process: [Linear, circumstantial, tangential, flight of ideas]
Thought content: [Delusions, obsessions, preoccupations — or WNL]
Perception: [Hallucinations — auditory, visual — or WNL]
Cognition: [Oriented x3/x4, attention, memory, concentration]
Insight: [Good/fair/poor]
Judgment: [Good/fair/poor]
Screening: [PHQ-9: X/27] [GAD-7: X/21] [Other: X]
Risk assessment: [Low/moderate/high — with supporting factors]
ASSESSMENT:
1. [Primary diagnosis] — [ICD-10 code]
[Status: improving/stable/worsening based on symptom trajectory]
2. [Comorbid diagnosis if applicable] — [ICD-10 code]
Risk level: [Low/Moderate/High] — [Justification based on
protective factors, risk factors, and clinical presentation]
PLAN:
1. [Therapy: modality (CBT/DBT/EMDR/psychodynamic), focus areas,
homework assigned]
2. [Medications: changes, refills, or new prescriptions with
rationale]
3. [Safety plan: if indicated — reviewed/updated/created]
4. [Referrals: psychiatry, group therapy, substance treatment]
5. [Patient education: psychoeducation topics covered]
6. [Follow-up: next session date, frequency]
7. [Crisis resources: provided if risk factors present]
3. Physical Therapy SOAP Note Template
SUBJECTIVE:
CC: "[Primary functional complaint]"
HPI: [Age]-year-old [sex] presents for [initial eval/session #X of Y]
for [condition/injury]. Patient reports pain at [location], currently
[X/10] on VAS. [Aggravating activities]. [Alleviating factors].
[Functional limitations: what the patient cannot do].
[Progress since last session: better/same/worse].
Goals reported: [Patient's functional goals in their words]
OBJECTIVE:
Observation: [Posture, gait pattern, assistive device use, guarding]
Palpation: [Tenderness, muscle tone, trigger points, swelling]
ROM: [Joint: Active X°/Passive X° (Normal: X°) — bilateral comparison]
Strength: [MMT grades by muscle group — X/5]
Special tests: [Test name: positive/negative — bilateral]
Functional tests: [Timed Up and Go: Xs, 6MWT: Xm, single-leg
stance: Xs, Berg Balance: X/56]
Neurological: [Sensation, reflexes, nerve tension tests]
Gait analysis: [Pattern, deviations, cadence, stride length]
Treatment provided:
- [Therapeutic exercise: type, sets, reps, resistance]
- [Manual therapy: technique, target tissue, duration]
- [Modalities: type, parameters, duration, location]
- [Neuromuscular re-education: activity, duration]
- [Patient education: topics, HEP modifications]
Patient response: [Tolerated well / required modifications / adverse]
ASSESSMENT:
1. [Primary diagnosis] — [ICD-10 code]
[Functional status: improving/plateau/declining]
2. [Rehab potential: good/fair/poor — with justification]
3. [Progress toward goals: % achieved, barriers identified]
4. [Treatment effectiveness: which interventions showing results]
PLAN:
1. [Continue/modify treatment plan: frequency X/week for X weeks]
2. [Progress exercises: specific modifications planned]
3. [Home exercise program: updated/maintained]
4. [Goals update: short-term and long-term goals with target dates]
5. [Coordination: MD communication, return to sport/work timeline]
6. [Next session focus: specific treatments planned]
4. Pediatrics SOAP Note Template
SUBJECTIVE:
CC: "[Chief complaint — from parent/guardian and/or child]"
HPI: [Age]-year-old [sex] brought in by [relationship to child] for
[symptom/reason]. Onset: [date/duration]. Associated symptoms: [list].
[Feeding/appetite changes]. [Activity level changes]. [Sleep pattern].
[School/daycare attendance impact].
Immunizations: [Up to date / Due for: list]
Growth/development: [Meeting milestones / Concerns noted]
Medications: [Current medications, OTC use]
Allergies: [Drug/food/environmental allergies]
Birth history: [If relevant — gestational age, complications]
OBJECTIVE:
Vitals: Temp [X°F], HR [X], RR [X], SpO2 [X%],
Weight [X kg] ([X percentile]), Height [X cm] ([X percentile]),
BMI [X percentile], Head circumference [X cm] ([X percentile])
General: [Alert, interactive, well-nourished / ill-appearing, fussy]
HEENT: [TMs, oropharynx, nasal mucosa, fontanelle if infant]
Neck: [Supple, lymphadenopathy]
Lungs: [CTA bilaterally, no retractions, no wheezing]
Cardiovascular: [RRR, no murmurs]
Abdomen: [Soft, non-tender, no organomegaly]
Skin: [Rashes, turgor, capillary refill]
Musculoskeletal: [Tone, symmetry, joint exam if relevant]
Neurological: [Appropriate for age, tone, reflexes]
Developmental: [Gross motor, fine motor, language, social — age-appropriate / delays noted]
ASSESSMENT:
1. [Primary diagnosis] — [ICD-10 code]
[Clinical reasoning based on exam and history]
2. [Growth/development status: on track / concern noted]
3. [Immunization status: current / catch-up needed]
PLAN:
1. [Medications: weight-based dosing — drug Xmg/kg, total dose,
route, frequency, duration]
2. [Anticipatory guidance: age-appropriate safety, nutrition, sleep]
3. [Immunizations administered: vaccine, lot#, site, VIS provided]
4. [Parent education: symptom management, return precautions]
5. [Referrals: developmental eval, specialist, early intervention]
6. [Follow-up: well-child schedule or illness recheck timing]
7. [Safety netting: when to call/go to ED — specific red flags]
5. Dermatology SOAP Note Template
SUBJECTIVE:
CC: "[Skin concern in patient's words]"
HPI: [Age]-year-old [sex] presents with [lesion/rash/concern] on
[anatomic location] for [duration]. Onset: [sudden/gradual].
[Pruritus/pain/bleeding/drainage: yes/no, severity].
[Spread/change in size or color]. [Prior treatments tried and results].
[Sun exposure history]. [Similar episodes in past].
[Family history of skin conditions/melanoma].
PMH: [Relevant — autoimmune conditions, immunosuppression]
Medications: [Current — note photosensitizing drugs]
Allergies: [Drug/topical/latex allergies]
Skin care routine: [Products used, frequency]
OBJECTIVE:
Skin examination:
- Location: [Anatomic site(s)]
- Morphology: [Macule/papule/plaque/nodule/vesicle/bulla/pustule/
patch/wheal/erosion/ulcer/crust/scale]
- Size: [X cm x X cm]
- Color: [Erythematous/hyperpigmented/hypopigmented/violaceous]
- Shape: [Round/oval/irregular/annular/linear/serpiginous]
- Border: [Well-defined/ill-defined/raised/flat]
- Distribution: [Localized/generalized/dermatomal/symmetric/
photo-distributed]
- Surface: [Smooth/rough/verrucous/keratotic]
- Consistency: [Firm/soft/fluctuant/indurated]
- Secondary changes: [Excoriation/lichenification/atrophy/scarring]
Dermoscopy: [Findings if performed — pigment network, globules,
streaks, vascular pattern]
Wood's lamp: [Findings if performed]
Biopsy: [Performed — site, technique (shave/punch/excisional),
specimen sent to pathology]
ASSESSMENT:
1. [Primary diagnosis] — [ICD-10 code]
[Clinical reasoning: morphology and distribution pattern supporting
diagnosis]
2. [Differential diagnoses considered and rationale for ruling out]
PLAN:
1. [Topical treatment: medication, strength, vehicle, application
instructions, quantity, refills]
2. [Systemic treatment if indicated: medication, dose, monitoring labs]
3. [Procedures: biopsy, cryotherapy, excision — site, technique]
4. [Pathology follow-up: expected timeline, plan for results]
5. [Sun protection counseling: SPF, reapplication, protective clothing]
6. [Photography: clinical photos taken for monitoring]
7. [Follow-up: timing — weeks/months, sooner if worsening]
6. Orthopedics SOAP Note Template
SUBJECTIVE:
CC: "[Musculoskeletal complaint]"
HPI: [Age]-year-old [sex/handedness] presents with [joint/region] pain
for [duration]. Mechanism of injury: [trauma/overuse/insidious onset].
Pain: [X/10], [sharp/dull/aching/burning], [constant/intermittent].
[Aggravating activities]. [Alleviating factors — rest, ice, elevation].
[Mechanical symptoms: locking, catching, giving way, instability].
[Swelling/bruising]. [Prior imaging or treatment].
[Functional impact: work, sports, ADLs].
PMH: [Prior surgeries, fractures, arthritis, osteoporosis]
Medications: [NSAIDs, analgesics, current use]
Occupational demands: [Physical labor level, sport/activity level]
OBJECTIVE:
Vitals: [If relevant — BP, HR]
Inspection: [Swelling, ecchymosis, deformity, atrophy, alignment,
surgical scars, skin integrity]
Palpation: [Point tenderness location, effusion, crepitus, warmth]
ROM: [Joint: Active X°/Passive X° (Normal: X°) — compare contralateral]
Strength: [MMT by muscle group — X/5, pain-limited vs. weakness]
Neurovascular: [Sensation, pulses, capillary refill — distal to injury]
Special tests:
- [Test 1: positive/negative]
- [Test 2: positive/negative]
- [Test 3: positive/negative]
Gait: [Normal / antalgic / Trendelenburg / other deviation]
Imaging reviewed:
- [X-ray: findings]
- [MRI: findings]
- [CT: findings if applicable]
ASSESSMENT:
1. [Primary diagnosis] — [ICD-10 code]
[Laterality: right/left], [acuity: acute/chronic/acute-on-chronic]
2. [Associated findings: effusion, instability grade, classification]
3. [Functional impact assessment]
PLAN:
1. [Conservative management: activity modification, bracing/splinting,
weight-bearing status]
2. [Medications: NSAIDs, analgesics, topicals — specific drug/dose]
3. [Physical therapy: referral with specific protocol/precautions]
4. [Injection: type (corticosteroid/HA/PRP), joint, approach, volume,
post-injection instructions]
5. [Imaging ordered: type, clinical indication]
6. [Surgical discussion: if indicated — procedure, risks/benefits
discussed, patient preference]
7. [Work/activity restrictions: specific limitations, duration]
8. [Follow-up: timing, criteria for earlier return]
7. Emergency Medicine SOAP Note Template
SUBJECTIVE:
CC: "[Chief complaint]"
HPI: [Age]-year-old [sex] presents to the ED via [ambulance/walk-in/
transfer] with [complaint] for [duration]. Onset: [time/date].
[Mechanism if trauma: details]. [Associated symptoms]. [Severity].
[What patient has tried]. [Pertinent positives and negatives].
PMH: [Conditions] PSH: [Surgeries]
Medications: [List with doses] Allergies: [NKDA or list with reaction]
SHx: [Tobacco/alcohol/drugs, occupation]
Last meal: [Time — relevant for procedural sedation/surgery]
Tetanus status: [Date of last — if wound/trauma]
EMS report: [Prehospital vitals, interventions, findings]
OBJECTIVE:
Vitals: BP [X/X], HR [X], RR [X], Temp [X°F], SpO2 [X%]
Triage: [ESI Level X]
General: [Appearance, distress level, GCS if applicable]
Primary survey: [A — airway patent/compromised, B — bilateral breath
sounds, C — pulses, hemorrhage control, D — neuro status, GCS,
E — exposure/environment]
[Focused exam by system — relevant to chief complaint]
HEENT: [Findings]
Cardiovascular: [Findings]
Respiratory: [Findings]
Abdomen: [Findings]
Musculoskeletal: [Findings — including neurovascular status if injury]
Neurological: [GCS, pupils, cranial nerves, motor/sensory, cerebellar]
Skin: [Wounds described: size, depth, contamination, neurovascular
status distal to injury]
Labs: [CBC, BMP, troponin, lactate, UA, coags, blood gas — results]
Imaging: [X-ray/CT/US findings and radiologist read if available]
ECG: [Rate, rhythm, intervals, ST changes, interpretation]
POC testing: [Rapid strep, flu, COVID, urine pregnancy — results]
ASSESSMENT:
1. [Primary diagnosis] — [ICD-10 code]
[Clinical reasoning: why this diagnosis over the differential]
2. [Differential diagnoses considered: list with reasoning]
3. [Acuity: critical/emergent/urgent/less urgent/nonurgent]
4. [Risk stratification: HEART score, Wells criteria, PERC, etc.]
PLAN:
1. [Treatment administered in ED: IV fluids, medications with doses
and times, procedures performed]
2. [Disposition: discharge / admit (floor/ICU/observation) / transfer]
3. [Prescriptions: medications, doses, quantity, refills]
4. [Discharge instructions: diagnosis-specific, activity restrictions]
5. [Follow-up: PCP in X days, specialist in X days, return to ED if
(specific red flags)]
6. [Pending results: labs/imaging to be followed up]
7. [Work/school note: dates of absence if applicable]
8. Neurology SOAP Note Template
SUBJECTIVE:
CC: "[Neurological complaint]"
HPI: [Age]-year-old [sex/handedness] presents with [symptom] for
[duration]. Onset: [sudden/gradual/episodic]. [Frequency if episodic].
[Triggers/aura if applicable]. [Progression: stable/worsening/
fluctuating]. [Associated symptoms: headache, dizziness, weakness,
numbness, vision changes, speech changes, seizures, gait
instability, cognitive changes].
[Functional impact: work, driving, ADLs].
[Prior neurological workup and results].
PMH: [Stroke, seizures, TBI, migraines, MS, neuropathy]
Medications: [Current neuro medications with doses and compliance]
FHx: [Neurological conditions — dementia, stroke, epilepsy, MS]
SHx: [Alcohol, recreational drugs, occupation, sleep habits]
OBJECTIVE:
Vitals: BP [X/X], HR [X]
Mental Status:
- Level of consciousness: [Alert/lethargic/obtunded]
- Orientation: [Person, place, time, situation]
- Attention: [Spell WORLD backward, serial 7s]
- Memory: [Immediate recall, short-term, long-term]
- Language: [Fluency, naming, repetition, comprehension]
- Visuospatial: [Clock draw, figure copy]
Cranial Nerves:
- I: [Not tested / olfaction intact]
- II: [Visual acuity, fields, fundoscopy, pupils (size, reactivity,
RAPD), color vision]
- III, IV, VI: [EOM intact, no nystagmus, no ptosis]
- V: [Facial sensation V1/V2/V3, masseter strength, corneal reflex]
- VII: [Facial symmetry, forehead wrinkle, smile, eye closure]
- VIII: [Hearing, Weber, Rinne, vestibular testing]
- IX, X: [Palate elevation, gag reflex, voice quality]
- XI: [SCM, trapezius strength]
- XII: [Tongue midline, no fasciculations]
Motor: [Tone, bulk, fasciculations, pronator drift]
- [Muscle group strength grading table — UE and LE bilateral]
Sensory: [Light touch, pinprick, vibration, proprioception, temperature
— dermatomal distribution]
Reflexes: [DTRs — biceps, triceps, brachioradialis, patellar, Achilles
— graded 0-4+, Babinski, Hoffman]
Coordination: [Finger-to-nose, heel-to-shin, rapid alternating
movements, Romberg]
Gait: [Casual, tandem, heel walk, toe walk, base width]
Imaging/studies reviewed: [MRI, CT, EEG, EMG/NCS, LP results]
ASSESSMENT:
1. [Primary diagnosis] — [ICD-10 code]
[Clinical reasoning: localization and mechanism]
2. [Differential diagnoses with reasoning]
3. [Disease status: new diagnosis / stable / progressing]
PLAN:
1. [Medications: neuro-specific drugs, dose titration schedule]
2. [Diagnostic workup: MRI, EEG, EMG/NCS, LP, bloodwork ordered]
3. [Referrals: neurosurgery, neuro-ophthalmology, PT/OT/speech]
4. [Lifestyle modifications: sleep hygiene, trigger avoidance, driving
restrictions]
5. [Patient education: disease-specific education, medication side
effects, seizure precautions if applicable]
6. [Follow-up: timing, bring seizure diary/headache log if applicable]
9. Cardiology SOAP Note Template
SUBJECTIVE:
CC: "[Cardiac complaint]"
HPI: [Age]-year-old [sex] with PMH of [cardiac history] presents with
[symptom] for [duration]. [Chest pain: OPQRST characterization].
[Dyspnea: exertional/at rest/orthopnea/PND — # of pillows].
[Palpitations: regular/irregular, duration, associated symptoms].
[Syncope/presyncope]. [Edema]. [Exercise tolerance: NYHA class/METs].
[Medication compliance]. [Dietary compliance: sodium, fluid].
[Weight changes]. [Device: pacemaker/ICD — last interrogation date].
Cardiac risk factors: [HTN, DM, HLD, smoking, family hx of premature
CAD, obesity, sedentary lifestyle]
OBJECTIVE:
Vitals: BP [X/X] (R arm) [X/X] (L arm if indicated), HR [X],
RR [X], SpO2 [X%], Weight [X lbs] (change from last: [+/- X lbs])
General: [Appearance, distress level]
Neck: [JVP X cm above sternal angle, carotid bruits, HJR]
Cardiovascular:
- PMI: [Location, character]
- Heart sounds: [S1, S2 — splitting, S3, S4]
- Murmurs: [Grade/6, location, radiation, timing, character]
- Rhythm: [Regular/irregular]
Respiratory: [Breath sounds, crackles (location, bilateral), wheezing]
Abdomen: [Hepatomegaly, ascites, pulsatile mass]
Extremities: [Edema (grade, location), pulses (DP, PT — bilateral),
capillary refill, skin temperature/color]
ECG: [Rate, rhythm, axis, intervals (PR, QRS, QTc), ST-T changes,
LVH/RVH criteria, comparison to prior]
Labs: [BNP/NT-proBNP, troponin, BMP (Cr, K, Na), lipid panel, HbA1c,
TSH]
Imaging: [Echo: EF X%, wall motion, valvular function, chamber sizes,
diastolic function. Stress test. Cath report if applicable]
Device interrogation: [Pacing %, lead impedance, battery, arrhythmia
episodes]
ASSESSMENT:
1. [Primary diagnosis] — [ICD-10 code]
[Status: compensated/decompensated, NYHA class, EF]
2. [Secondary diagnoses with ICD-10 codes]
3. [Risk stratification: ASCVD risk %, CHA2DS2-VASc, HAS-BLED]
PLAN:
1. [Medications: GDMT optimization — specific drugs, target doses,
titration plan]
2. [Diagnostics ordered: echo, stress test, Holter, cath, CT-A]
3. [Lifestyle: sodium <2g/day, fluid restriction, daily weights,
exercise prescription, smoking cessation]
4. [Device management: programming changes, follow-up schedule]
5. [Anticoagulation: drug, dose, INR target if warfarin, monitoring]
6. [Referrals: EP, CT surgery, cardiac rehab, dietary counseling]
7. [Follow-up: timing, weight gain threshold for earlier contact]
10. Chiropractic SOAP Note Template
SUBJECTIVE:
CC: "[Musculoskeletal complaint]"
HPI: [Age]-year-old [sex] presents with [region] pain for [duration].
Onset: [trauma/repetitive/insidious]. Pain: [X/10], [character].
[Radiation pattern]. [Aggravating: sitting, standing, bending, lifting].
[Alleviating: position changes, ice, heat, OTC meds].
[Functional limitations: work, sleep, ADLs, exercise].
[Prior chiropractic/medical treatment and response].
[Progress since last visit if established patient: better/same/worse].
Daily activities affected: [Specific limitations reported]
OBJECTIVE:
Posture: [Anterior/lateral view — head position, shoulder level,
pelvic tilt, spinal curves, extremity alignment]
Gait: [Pattern, deviations, antalgic component]
Palpation: [Segmental tenderness, muscle hypertonicity, trigger points
— location and severity]
ROM: [Cervical/thoracic/lumbar — flexion, extension, lateral flexion,
rotation — degrees, pain response]
Orthopedic tests:
- [Test 1: positive/negative/equivocal]
- [Test 2: positive/negative/equivocal]
- [Test 3: positive/negative/equivocal]
Neurological: [DTRs, dermatome sensation, myotome strength, Babinski]
Muscle strength: [MMT relevant muscle groups — X/5]
Subluxation/joint dysfunction findings:
- [Segment: direction of misalignment, motion restriction, tissue
texture change, tenderness]
Imaging: [X-ray findings if taken — alignment, disc space, degeneration]
Treatment provided:
- Chiropractic adjustment: [Segments adjusted, technique (Diversified/
Gonstead/Activator/Thompson/Flexion-Distraction), patient position]
- Soft tissue therapy: [Technique, target muscles, duration]
- Modalities: [E-stim/ultrasound/cold laser — parameters, location,
duration]
- Therapeutic exercises: [Prescribed — type, sets, reps]
Patient tolerance: [Tolerated well / adverse response noted]
ASSESSMENT:
1. [Primary diagnosis] — [ICD-10 code]
[Spinal region, laterality, acuity]
2. [Subluxation complex: segments involved]
3. [Functional improvement: compared to initial presentation or last
visit — % improvement, objective measures]
4. [Prognosis: good/fair/guarded]
PLAN:
1. [Treatment frequency: X visits/week for X weeks, then reassess]
2. [Home care: ice/heat protocol, ergonomic modifications, stretches]
3. [Exercise prescription: specific exercises for home program]
4. [Lifestyle modifications: workstation setup, sleeping position,
lifting technique]
5. [Re-examination: scheduled at visit #X for progress evaluation]
6. [Referral: if indicated — MD, PT, imaging]
7. [Next visit: date and planned treatment focus]
SOAP Note Examples — Filled Out by Specialty
The templates above give you the structure. The examples below show you what a completed SOAP note looks like with realistic clinical data. Use these as reference models when writing your own notes.
Example 1: Primary Care — Acute Low Back Pain
SUBJECTIVE:
CC: "My lower back has been killing me for about a week."
HPI: 42-year-old male presents with lower back pain for 7 days.
Onset: gradual, began after moving furniture last Saturday. Location:
bilateral lumbar region, no radiation to legs. Character: dull,
aching, with sharp pain on bending forward. Severity: 6/10 at rest,
8/10 with activity. Aggravating: bending, lifting, prolonged sitting.
Alleviating: lying flat, ibuprofen 400mg (partial relief). No
numbness, tingling, leg weakness, bowel or bladder changes.
No fever, no weight loss. No prior episodes.
ROS: Negative for fever, urinary symptoms, leg weakness, saddle
anesthesia. Positive for disturbed sleep due to pain.
PMH: Hypertension (controlled), no prior surgeries.
Medications: Lisinopril 10mg daily, ibuprofen 400mg PRN.
Allergies: NKDA.
SHx: Office worker, no tobacco, social alcohol. Sedentary lifestyle.
FHx: Father — osteoarthritis. No ankylosing spondylitis or RA.
OBJECTIVE:
Vitals: BP 128/82, HR 76, RR 14, Temp 98.4°F, SpO2 99%,
Weight 198 lbs, BMI 28.4
General: Alert, oriented, mild discomfort with position changes.
Spine: No visible deformity or skin changes. Tenderness to palpation
over bilateral paraspinal muscles L3-L5. No midline spinous process
tenderness. Paravertebral muscle spasm bilateral.
ROM: Lumbar flexion limited to ~50% with pain, extension 75%,
lateral flexion mildly reduced bilaterally.
Neurological: Straight leg raise negative bilaterally. Sensation
intact L2-S1 dermatomes bilateral. Motor strength 5/5 bilateral
hip flexion, knee extension, ankle dorsiflexion, and plantarflexion.
Patellar reflexes 2+ bilateral. Achilles reflexes 2+ bilateral.
Gait: Mildly antalgic, no foot drop.
No saddle anesthesia. Rectal tone not assessed (no red flags).
ASSESSMENT:
1. Acute lumbar strain — M54.50 (Low back pain, unspecified)
Clinical reasoning: Mechanical onset (lifting), bilateral
paraspinal muscle spasm, no neurological deficits, negative SLR.
No red flags for fracture, infection, or cauda equina syndrome.
2. Hypertension — I10 (Essential hypertension) — well-controlled,
continue current regimen.
PLAN:
1. Naproxen 500mg PO BID with food x 10 days (switch from ibuprofen
for longer duration coverage). Avoid acetaminophen overuse.
2. Cyclobenzaprine 10mg PO at bedtime PRN x 7 days for muscle spasm.
3. Activity modification: avoid heavy lifting >15 lbs for 2 weeks.
Encouraged to remain active — walking 20 min daily. No bed rest.
4. Ice 20 min on/off for first 48 hours, then alternate with heat.
5. Patient education: discussed natural history (90% improve within
6 weeks), proper lifting mechanics, importance of core
strengthening. Handout provided.
6. No imaging at this time — no red flags, first episode, <6 weeks.
7. Follow-up: 2 weeks or sooner if develops leg weakness, numbness,
bowel/bladder changes, or symptoms worsen significantly.
If no improvement at 4 weeks, will order lumbar X-ray and
consider PT referral.
Example 2: Mental Health — Therapy Follow-Up (Depression)
SUBJECTIVE:
CC: "I'm doing a little better this week but still struggling."
HPI: 34-year-old female presents for therapy session #8, follow-up
for major depressive disorder, moderate. Patient reports slight
improvement in mood since starting sertraline 50mg 3 weeks ago.
Sleep: improved from 4 hours to 6 hours, still waking early at 4 AM.
Appetite: slightly improved, eating 2 meals/day (was 1). Energy:
still low but able to complete basic self-care consistently.
Concentration: difficulty at work, missed 2 deadlines this week.
Reports using journaling (assigned homework) 4 of 7 days — found
it "somewhat helpful" for identifying negative thought patterns.
Stressors: ongoing conflict with supervisor about performance.
Financial stress due to reduced work productivity.
Suicidal ideation: Denies current SI. Reports passive thought
2 weeks ago ("I just don't want to be here") but no plan, intent,
or means. Endorses protective factors: 8-year-old daughter,
supportive mother, commitment to treatment.
Homicidal ideation: Denied.
Substance use: Glass of wine 2-3x/week, denied increased use.
OBJECTIVE:
Appearance: Casually dressed, adequate hygiene, mild psychomotor
slowing. Made intermittent eye contact. Less tearful than prior session.
Behavior: Cooperative, engaged in session, willing to participate
in interventions.
Speech: Normal rate, low volume, spontaneous but brief.
Mood: "A little better but still heavy."
Affect: Mildly constricted range, congruent with stated mood,
tearful when discussing work conflict. Brighter affect when
discussing daughter.
Thought process: Linear and goal-directed. Mild rumination on
work performance.
Thought content: No delusions. Mild negative self-evaluation
("I'm falling behind everyone"). No current SI/HI.
Perception: No hallucinations.
Cognition: Oriented x4, attention mildly impaired (required
redirection 2x during session), memory intact.
Insight: Fair — recognizes connection between thoughts and mood
but struggles to interrupt patterns.
Judgment: Fair — attending appointments, taking medication, engaged
in therapy homework.
PHQ-9: 14/27 (moderate) — down from 18 at session #6.
GAD-7: 8/21 (mild anxiety) — stable.
Risk assessment: Low acute risk. History of passive SI (2 weeks ago,
resolved). Protective factors: child, family support, treatment
engagement, no substance abuse escalation, no access to lethal means.
ASSESSMENT:
1. Major depressive disorder, single episode, moderate — F32.1
Status: Mildly improving. PHQ-9 decreased from 18 to 14 over 2
sessions. Sleep and appetite improving. Concentration remains
impaired. Medication response emerging at 3 weeks.
2. Generalized anxiety disorder — F41.1
Status: Stable, mild severity. Contributing to work performance
concerns.
Risk level: Low — no current SI, protective factors present,
treatment engaged, medication response beginning.
PLAN:
1. Continue CBT: Today's session focused on cognitive restructuring
— identified 3 core negative beliefs about competence ("I always
fail," "Everyone is ahead of me," "I'm going to get fired").
Practiced reframing with evidence-based alternative thoughts.
Homework: thought record 5 days/week targeting work-related
automatic thoughts.
2. Medication: Continue sertraline 50mg daily. Discuss dose increase
to 100mg with psychiatrist at next med management appointment
(April 15) if PHQ-9 remains >10 at 6-week mark.
3. Behavioral activation: Schedule 3 pleasurable activities this week
(patient selected: walk with daughter, cooking a new recipe,
calling a friend). Track mood before and after in journal.
4. Sleep hygiene reinforced: consistent wake time 6:30 AM, no screens
30 min before bed, relaxation exercise (progressive muscle
relaxation audio provided).
5. Safety: No safety plan update needed at this time. Patient aware
of crisis line (988) and has mother as emergency contact.
6. Next session: April 13, 2026, 2:00 PM. Focus: behavioral
activation review and introducing graded task assignment for
work productivity.
Example 3: Physical Therapy — Knee Rehabilitation
SUBJECTIVE:
CC: "My knee is feeling stronger but still swells after exercise."
HPI: 28-year-old female, session #10 of 16 for right ACL
reconstruction rehab (hamstring autograft, 8 weeks post-op). Reports
pain 2/10 at rest, 4/10 with stairs. Swelling: mild after PT
exercises, resolves with ice within 2 hours. Able to walk without
brace for short distances at home. Still using crutch for longer
walks. Reports completing HEP 6/7 days. Sleeping through the night
without pain. Goals: return to recreational soccer by month 6.
OBJECTIVE:
Observation: Mild right quadriceps atrophy vs. left. No visible
effusion at rest. Well-healed portal sites. Normal patellar tracking.
Gait: Independent without assistive device for 200 ft. Mild right
quadriceps avoidance pattern. No Trendelenburg.
Palpation: Mild joint line tenderness medial. No warmth. Trace
effusion on sweep test.
ROM:
- Right knee flexion: Active 118°/Passive 124° (Left: 140°)
- Right knee extension: Active 0°/Passive 0° (Full, symmetric)
Strength (MMT):
- Right quadriceps: 4-/5 (Left: 5/5)
- Right hamstrings: 4/5 (Left: 5/5)
- Right hip abductors: 4+/5
Special tests: Lachman: Grade 1A (firm endpoint) — expected post-ACL-R.
Pivot shift: negative. No varus/valgus instability.
Functional tests:
- Single-leg stance right: 22 seconds (Left: 30+ seconds)
- Step-down test: 3/10 quality — mild medial knee collapse
Treatment provided:
- Stationary bike warm-up: 10 min, low resistance
- Quad sets: 3x15 with biofeedback
- Straight leg raises 4-way: 3x12 with 3 lb ankle weight
- Mini squats 0-60°: 3x12, focus on form/alignment
- Step-ups (4-inch): 3x10 each leg
- Balance board: 3x60 seconds bilateral, 3x30 seconds single-leg R
- Hamstring curls (prone): 3x12 with 5 lb resistance
- Patellar mobilization: superior/inferior, 3 min
- Cryotherapy: 15 min with compression wrap post-exercise
Patient response: Tolerated well. No increase in pain or effusion
during session. Required cueing for knee valgus on step-ups.
ASSESSMENT:
1. Status post right ACL reconstruction with hamstring autograft —
S83.511D (Sprain of anterior cruciate ligament, right knee,
subsequent encounter)
Week 8: Progressing appropriately. Full extension achieved.
Flexion at 84% of contralateral. Quad strength improving but
remains primary deficit. Trace effusion managed with ice.
2. Rehab potential: Good. Patient compliant with HEP, motivated,
age-appropriate healing. On track for phase 3 (running) at
week 12-14 pending quad strength >70% contralateral.
3. Goal progress: 4 of 6 short-term goals met (full extension,
independent gait <200ft, pain <3/10 at rest, HEP compliance).
2 remaining (flexion >130°, quad MMT 4+/5).
PLAN:
1. Continue PT 2x/week for 6 weeks (sessions 11-22).
2. Progress closed-chain strengthening: increase step-up height to
6 inches, add wall slides to 70° with 5-sec hold.
3. Initiate single-leg press (leg press machine) at 50% body weight.
4. Begin neuromuscular control: lateral shuffles with band, cone drills.
5. HEP update: add single-leg mini squats (3x8) and eccentric
hamstring lowers on step.
6. Ice 15 min post-exercise and after HEP.
7. Re-evaluate flexion ROM and quad strength at session #12.
8. Communicate with surgeon: progress note sent, inquire about
running clearance timeline.
9. Next session: Wednesday — focus on quad strengthening and
neuromuscular control.
Example 4: Pediatrics — Well-Child Visit (4-Year-Old)
SUBJECTIVE:
CC: "Here for his 4-year-old checkup."
HPI: 4-year-old male brought in by mother for well-child visit.
No acute concerns today. Mother reports he is "doing great in
preschool" — started 3 months ago, adjusting well, has made friends.
Diet: Eats well, 3 meals and 2 snacks daily, drinks milk (16 oz/day),
limited juice. Bowel/bladder: fully toilet trained day and night,
no constipation. Sleep: 10-11 hours/night, consistent bedtime 7:30 PM,
no nighttime awakenings. Screen time: ~1 hour/day (PBS shows, tablet
games).
Development per parent: Speaks in full sentences (5-6 words), tells
stories, knows first and last name, counts to 20, recognizes some
letters. Draws a person with 3+ body parts. Hops on one foot.
Dresses self with help for buttons. Plays cooperatively with peers.
Immunizations: Up to date through 18-month series. Due for 4-year
boosters today.
PMH: 2 episodes of AOM (last at age 2), no surgeries, no
hospitalizations. Allergies: NKDA. Medications: None.
FHx: Father — asthma. Mother — seasonal allergies. No developmental
delays in siblings.
OBJECTIVE:
Vitals: Temp 98.2°F, HR 92, RR 20, BP 96/58, SpO2 100%
Weight: 36.2 lbs (16.4 kg) — 45th percentile
Height: 40.5 in (102.9 cm) — 50th percentile
BMI: 15.6 — 45th percentile
Vision screen: 20/30 bilateral (pass)
Hearing screen: Pass bilateral (pure tone audiometry)
General: Well-nourished, well-developed, active, cooperative,
interactive. Happy and playful.
HEENT: Normocephalic, TMs clear bilateral with normal landmarks,
oropharynx clear, dentition appropriate with no caries visible.
Neck: Supple, no lymphadenopathy.
Cardiovascular: RRR, no murmurs.
Respiratory: CTA bilaterally, no distress.
Abdomen: Soft, non-tender, no organomegaly.
GU: Normal male external genitalia, testes descended bilaterally.
Musculoskeletal: Normal gait, full ROM, no scoliosis.
Skin: Clear, no rashes or bruising patterns.
Neurological: Age-appropriate — good balance, coordination, follows
multi-step commands. Speech clear and intelligible.
Developmental assessment (direct observation):
- Gross motor: Hops on one foot x3, throws ball overhand, climbs
- Fine motor: Copies circle and cross, draws person (head, body, legs)
- Language: Speaks in 5-6 word sentences, tells short story, names
4 colors, counts to 12 (observed)
- Social: Cooperative play with examiner, shares toys, takes turns
ASSESSMENT:
1. Well-child visit, 4 years — Z00.129
Growth: Tracking 45-50th percentiles, proportionate, BMI healthy.
Development: Meeting all milestones for age across gross motor,
fine motor, language, and social domains. No concerns.
Vision and hearing: Pass.
2. Immunizations: Due for 4-year boosters.
PLAN:
1. Immunizations administered today:
- DTaP (Daptacel, Lot #C4321, 0.5mL IM left deltoid)
- IPV (IPOL, Lot #P8765, 0.5mL IM right deltoid)
- MMR (M-M-R II, Lot #M2345, 0.5mL SC left upper arm)
- Varicella (Varivax, Lot #V6789, 0.5mL SC right upper arm)
VIS provided for each, reviewed with mother. Consent obtained.
Monitored 15 minutes post-injection — no adverse reaction.
2. Anticipatory guidance discussed:
- Car safety: Forward-facing car seat with harness until outgrows
weight/height limits, then booster seat
- Water safety: Never swim without adult supervision, begin
swim lessons
- Nutrition: Continue balanced diet, limit juice to 4 oz/day
- Screen time: 1 hour/day limit appropriate, encourage active play
- Dental: Brush 2x/day with fluoride toothpaste, dental visit q6mo
- Preschool readiness: social skills on track, encourage reading
3. Next well-child visit: Age 5 (kindergarten readiness), annual
influenza vaccine in fall.
4. Return sooner for any acute concerns.
Example 5: Dermatology — Suspicious Mole Evaluation
SUBJECTIVE:
CC: "I noticed this mole on my back changed color."
HPI: 56-year-old male presents for evaluation of a pigmented lesion
on the right upper back. Wife noticed the mole "got darker" and
"looks different" over the past 3 months. Patient reports no pain,
itching, or bleeding from the lesion. No prior biopsy of this lesion.
Has >50 moles total. No personal history of melanoma or non-melanoma
skin cancer.
Sun exposure: History of 3-4 blistering sunburns as a teenager.
Worked construction outdoors for 15 years. Does not use sunscreen
regularly. No tanning bed use.
FHx: Mother — basal cell carcinoma (age 68). No melanoma in family.
PMH: Type 2 diabetes (metformin), hypertension (amlodipine).
Medications: Metformin 1000mg BID, amlodipine 5mg daily.
Allergies: Sulfa — rash.
OBJECTIVE:
Skin examination:
Target lesion — right upper back (scapular region):
- Morphology: Asymmetric papule with irregular border
- Size: 8mm x 6mm (patient reports was ~5mm previously)
- Color: Variegated — dark brown, light brown, with focal area of
blue-black pigmentation at 2 o'clock position
- Border: Irregular, scalloped, with notching at 7 o'clock position
- Surface: Mostly flat with raised central component
- ABCDEs: Asymmetry (+), Border irregularity (+), Color variation (+),
Diameter >6mm (+), Evolution (+)
Dermoscopy:
- Atypical pigment network: irregular mesh with thick brown lines
and irregular spacing
- Blue-white veil: focal area corresponding to blue-black zone
- Irregular dots/globules at periphery
- Regression structures: focal areas of peppering
- No typical benign pattern identified
Full-body skin exam:
- >50 melanocytic nevi, mostly <6mm, clinically benign pattern
- 3 additional atypical-appearing nevi flagged for monitoring (left
shoulder, right flank, left calf) — photographed
- 2 actinic keratoses noted on bilateral forearms
- No other suspicious lesions
ASSESSMENT:
1. Atypical melanocytic lesion, right upper back — suspicious for
melanoma — D48.5 (Neoplasm of uncertain behavior, skin)
ABCDEs criteria met (4/5 positive). Dermoscopy features concerning
for invasive melanoma (atypical network, blue-white veil,
regression). Biopsy required for definitive diagnosis.
2. Atypical nevi x3 — D22 series (Melanocytic nevi)
Flagged for monitoring with baseline photography.
3. Actinic keratoses, bilateral forearms x2 — L57.0
PLAN:
1. Excisional biopsy of right upper back lesion performed today:
- Technique: Elliptical excision with 2mm clinical margins
- Size: 14mm x 8mm ellipse, full-thickness to subcutaneous fat
- Hemostasis: electrocautery
- Closure: 4-0 nylon interrupted sutures x6
- Specimen: placed in formalin, sent to dermatopathology
- Wound care instructions provided: keep dry 24 hours, then clean
with soap and water daily, apply petroleum jelly and bandage,
suture removal in 10-14 days
2. Pathology follow-up: results expected 5-7 business days. Patient
will be called with results. If melanoma confirmed, will schedule
wide local excision with appropriate margins based on Breslow depth.
3. Actinic keratoses: treated with cryotherapy (liquid nitrogen,
2 freeze-thaw cycles each, ~10 seconds per cycle).
4. Atypical nevi: baseline clinical photographs taken of 3 lesions.
Monitor at 3-month intervals with serial photography.
5. Sun protection counseling: daily SPF 30+ broad-spectrum sunscreen,
reapply every 2 hours outdoors, UPF protective clothing, avoid
peak UV hours 10AM-4PM, monthly self-skin exam education provided.
6. Follow-up: 10 days for suture removal and pathology results.
Full-body skin exam q6 months given risk profile (>50 nevi,
sun damage history, atypical nevi).
Example 6: Emergency Medicine — Chest Pain Evaluation
SUBJECTIVE:
CC: "Chest pain that started an hour ago."
HPI: 58-year-old male presents to ED via EMS with substernal chest
pain for approximately 1 hour. Onset: sudden, while watching
television. Character: pressure, "like someone sitting on my chest."
Severity: 8/10. Radiation to left arm and jaw. Associated symptoms:
diaphoresis, nausea (no vomiting), mild dyspnea. No syncope.
No recent trauma. No prior similar episodes.
Aggravating: nothing identified. Alleviating: nil so far.
Prehospital: EMS administered aspirin 324mg PO, sublingual
nitroglycerin 0.4mg x1 — pain reduced from 8/10 to 5/10.
12-lead ECG in field: ST elevations noted anterior leads (per EMS).
PMH: HTN (on lisinopril), hyperlipidemia (on atorvastatin), type 2
DM (on metformin). Former smoker — quit 5 years ago (30 pack-year hx).
No prior MI, PCI, or CABG.
Medications: Lisinopril 20mg daily, atorvastatin 40mg daily,
metformin 1000mg BID, aspirin 81mg daily.
Allergies: NKDA.
Last meal: 3 hours ago.
FHx: Father — MI at age 52. Mother — HTN, alive.
OBJECTIVE:
Vitals: BP 156/94, HR 96, RR 22, Temp 98.6°F, SpO2 96% on RA
Triage: ESI Level 2
General: Alert, oriented, diaphoretic, moderate distress, clutching
chest.
HEENT: Pale. No JVD.
Cardiovascular: Tachycardic, regular rhythm, no murmurs, no S3/S4.
Peripheral pulses 2+ bilaterally. No peripheral edema.
Respiratory: Tachypneic. CTA bilaterally, no crackles, no wheezing.
Abdomen: Soft, non-tender, non-distended.
Extremities: Warm, no cyanosis, no edema. Capillary refill <2 sec.
Neurological: GCS 15, alert, oriented x4, no focal deficits.
ECG (12-lead, ED):
- Rate 96 bpm, normal sinus rhythm
- ST elevation 2-3mm in V1-V4 (anterior leads)
- Reciprocal ST depression in leads II, III, aVF
- No prior ECG for comparison
Labs (rapid):
- Troponin I: 0.82 ng/mL (elevated; normal <0.04)
- BMP: Na 140, K 4.2, Cr 1.0, Glucose 186
- CBC: WBC 11.2, Hgb 14.8, Plt 232
- Coags: PT 12.1, INR 1.0
- BNP: 89 pg/mL
Chest X-ray: No cardiomegaly, no pulmonary edema, no pneumothorax,
no infiltrates.
ASSESSMENT:
1. ST-elevation myocardial infarction (STEMI), anterior wall — I21.02
(STEMI involving left anterior descending coronary artery)
Clinical reasoning: Classic presentation (substernal pressure with
radiation, diaphoresis, cardiac risk factors), anterior ST
elevations V1-V4 with reciprocal inferior depression, elevated
troponin (0.82). Consistent with acute LAD territory MI.
HEART score: 9 (high risk).
2. Hypertension, uncontrolled in acute setting — I10
3. Type 2 diabetes mellitus — E11.9
4. Hyperlipidemia — E78.5
PLAN:
1. STEMI protocol activated — cardiac catheterization lab notified,
door-to-balloon time initiated.
2. Medications administered in ED:
- Aspirin 324mg PO (given by EMS — documented)
- Ticagrelor 180mg PO loading dose — given at [time]
- Heparin 60 units/kg IV bolus (5,500 units) — given at [time]
- Heparin drip 12 units/kg/hr initiated
- Nitroglycerin drip started at 10 mcg/min, titrate for chest
pain, hold if SBP <100
- Metoprolol 5mg IV — given at [time] (HR >60, SBP >120, no CHF)
- Morphine 4mg IV — given at [time] for ongoing pain
3. Hold metformin (contrast dye risk with cath).
4. Continuous cardiac monitoring, 2 large-bore IVs, O2 via NC at
2L/min for SpO2 96%.
5. Disposition: Emergent cardiac catheterization for primary PCI.
Interventional cardiology (Dr. [Name]) notified and en route.
6. Family notified, updated on plan. Consent for cardiac
catheterization obtained.
7. Post-PCI: Admit to cardiac ICU for monitoring, serial troponins
q6h, repeat ECG post-intervention, echocardiogram within 24 hours.
How to Write a SOAP Note — Step-by-Step Guide
Whether you are a medical student learning the format for the first time or an experienced clinician looking to improve your documentation efficiency, the following process works across every specialty.
Step 1: Start Before the Patient Leaves
The biggest documentation mistake is waiting until the end of the day to write notes. By then, clinical details blur together. Start the Subjective section during the patient interview — either with brief shorthand notes or by using an AI scribe that captures the conversation in real time.
Step 2: Document the Subjective Section First
Begin with the chief complaint in the patient's own words — use direct quotes. Then document the HPI using a structured framework (OLDCARTS: Onset, Location, Duration, Character, Aggravating, Relieving, Timing, Severity). Include pertinent ROS findings, medications, allergies, and relevant social/family history. Omit irrelevant system reviews — document what supports or rules out your clinical thinking.
Step 3: Record Objective Findings Systematically
Document vital signs first, then physical exam findings organized by system. Include only systems you examined — do not template-stamp systems you did not assess. Record screening tool scores (PHQ-9, GAD-7, VAS) and diagnostic results with specific values, not just "normal" or "abnormal."
Step 4: Write the Assessment with Clinical Reasoning
State each diagnosis with the ICD-10 code. For new problems, document your differential and explain why you selected the primary diagnosis over alternatives. For established problems, note whether the condition is improving, stable, or worsening and what data supports that conclusion. This is the section auditors scrutinize — make your reasoning explicit.
Step 5: Make the Plan Actionable
Every Plan item should be specific enough that a covering provider could execute it without calling you. "Continue medications" is inadequate. "Continue metformin 1000mg BID, check HbA1c in 3 months, follow up in 3 months or sooner if fasting glucose consistently >180" is defensible.
Step 6: Review for Completeness and Compliance
Before signing, verify: (1) the Assessment is supported by the S and O data, (2) the Plan addresses every problem in the Assessment, (3) the complexity of your documentation supports the E/M code billed, and (4) no copy-forward errors from previous notes.
The 60-second self-audit. After finishing a note, ask yourself three questions: (1) Could another provider understand the clinical picture and execute the plan without calling me? (2) Does the assessment logically follow from the subjective and objective data? (3) Would this note withstand an audit? If you answer "no" to any of these, the note needs revision.
AI SOAP Note Generators — Skip Templates Entirely
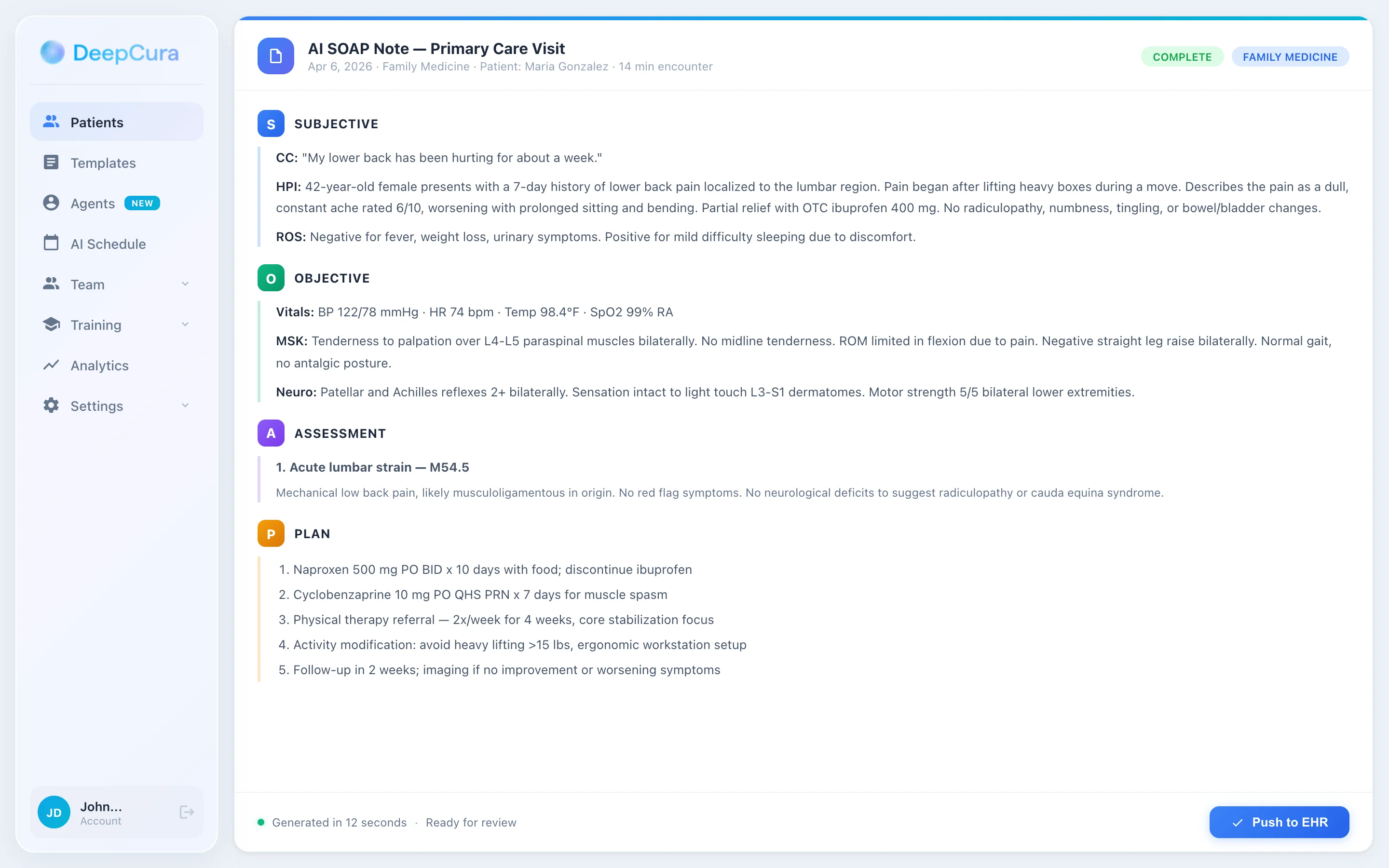
Templates save structure time. AI eliminates documentation time altogether. An AI SOAP note generator listens to the patient encounter and automatically produces a complete, structured SOAP note — with accurate S, O, A, and P sections — in seconds.
How AI SOAP Note Generation Works
- Ambient listening — The AI scribe (running on your phone, tablet, or desktop) listens to the natural conversation between you and the patient. No special dictation or keywords required.
- Real-time structuring — The AI identifies which parts of the conversation map to Subjective (patient's complaints, history), Objective (your exam findings as you dictate them), Assessment (your diagnostic reasoning), and Plan (your treatment decisions).
- Draft generation — Within seconds of the encounter ending, a complete SOAP note appears in your queue. The note follows your preferred format, uses correct medical terminology, and includes relevant ICD-10 codes.
- Provider review — You review the draft, make any edits, and approve. The approved note is pushed directly to your EHR with one click — no copy-paste, no re-typing.
Why Clinicians Are Switching from Templates to AI
| Templates | AI SOAP Note Generator | |
|---|---|---|
| Time per note | 10-15 minutes | 30 seconds (review only) |
| Copy-paste risk | High (stale data from prior notes) | None (generated fresh per encounter) |
| Coding accuracy | Manual ICD-10 lookup | Auto-suggested codes from clinical context |
| EHR integration | Manual entry | One-click write-back |
| Customization | One-size-fits-all | Adapts to your style, specialty, and templates |
| Cost | Free (but time cost: 2-3 hours/day) | $129/month (saves 2-3 hours/day) |
DeepCura — The All-in-One AI SOAP Note Generator
DeepCura goes beyond basic SOAP note generation. It is a complete clinical AI platform that includes:
- AI Medical Scribe — ambient SOAP note generation from any encounter type (in-person, telehealth, phone). Supports 50+ specialties with specialty-specific note templates. Writes to your EHR (Athena, Epic, eClinicalWorks, DrChrono, AdvancedMD, and more) with one click.
- AI Receptionist — answers patient calls 24/7, books appointments, collects payments, sends intake forms, and handles prescription refill requests. No more missed calls or voicemail backlog. Read our guide to the Best AI Medical Receptionist for more.
- AI Fax Management — automatically reads, summarizes, and routes incoming faxes. No more paper sorting.
- AI Billing Assistant — suggests CPT codes based on your documentation complexity, flags undercoding, and checks modifier accuracy.
- AI Clinical Chat — ask clinical questions, get treatment guidelines, drug interaction checks, and differential diagnosis support. See our Best ChatGPT for Doctors guide.
$129/month per provider. No per-note fees. No usage limits. Most AI scribe tools charge per minute or per encounter — DeepCura includes unlimited encounters, all features, and full EHR integration in one flat rate.
For detailed comparisons with other AI documentation tools, see our reviews of Freed AI, Heidi Health, and the full Best AI Medical Scribes in 2026 ranking.
See DeepCura in Action
Watch how DeepCura generates a complete SOAP note from a live patient encounter — ambient listening, structured output, and one-click EHR write-back.

Common SOAP Note Mistakes to Avoid
Even experienced clinicians make documentation errors that create audit risk or compromise patient care continuity. Here are the eight most frequent SOAP note mistakes and how to avoid them.
-
Mixing Subjective and Objective data. Patient-reported symptoms belong in S. Your exam findings and measurements belong in O. "Patient appears anxious" is Objective (your observation). "Patient reports feeling anxious" is Subjective (their words). Mixing the two confuses the clinical narrative and can trigger audit flags.
-
Assessment without reasoning. Writing "HTN" without documenting whether it is controlled, uncontrolled, or newly diagnosed — and what data supports that determination — leaves the note clinically incomplete. Auditors look for the logical connection between your S/O data and your Assessment.
-
Vague Plan items. "Follow up as needed" and "continue current medications" do not constitute a plan. Specify drug names, doses, frequencies, and follow-up timeframes. A clear Plan protects you legally and ensures continuity if another provider sees the patient.
-
Copy-forward contamination. Templating or copying from a previous note without updating findings is one of the top audit triggers. Every SOAP note must reflect the current encounter. If you use a template, verify every pre-populated field before signing.
-
Underdocumentation of medical decision-making. The Assessment and Plan sections drive E/M coding. A complex encounter documented with a sparse Assessment and one-line Plan will be downcoded, costing the practice revenue. Document your reasoning, differential, and the complexity of decisions made.
-
Omitting negative findings. Pertinent negatives are as important as positives. "No chest pain, no dyspnea, no syncope" in a cardiac evaluation demonstrates that you considered and ruled out relevant symptoms. Without them, an auditor cannot tell whether you asked.
-
Not documenting patient education. The Plan section should include what you discussed with the patient — especially for medication changes, lifestyle modifications, and safety netting instructions. This documents informed consent and shared decision-making.
-
Signing late. Notes signed days after the encounter are a red flag for auditors and raise questions about accuracy. Best practice is to complete and sign notes within 24 hours — ideally immediately after the encounter using an AI scribe that generates the draft in real time.
Frequently Asked Questions
What does SOAP stand for in a SOAP note?
SOAP stands for Subjective, Objective, Assessment, and Plan. The Subjective section captures the patient's reported symptoms and history. The Objective section documents the clinician's examination findings, vital signs, and test results. The Assessment contains the clinical diagnosis or differential with reasoning. The Plan outlines treatment decisions, medications, referrals, and follow-up instructions. This four-part structure was developed by Dr. Lawrence Weed in the 1960s and remains the most widely used clinical documentation format worldwide.
How do you write a SOAP note for the first time?
Start with the Subjective section by documenting the chief complaint in the patient's own words, then use the OLDCARTS mnemonic (Onset, Location, Duration, Character, Aggravating, Relieving, Timing, Severity) to structure the history of present illness. Move to Objective and record vital signs followed by physical exam findings organized by system. In the Assessment, state your diagnosis with the ICD-10 code and explain your clinical reasoning. In the Plan, list specific medications with doses, ordered tests, referrals, patient education topics, and follow-up timing. Review the completed examples in this guide to see the format in practice.
What is the difference between a SOAP note and a progress note?
A SOAP note is a type of progress note — specifically, one structured in the Subjective, Objective, Assessment, and Plan format. A progress note is a broader term for any documentation of a patient encounter, which may follow different formats such as DAP (Data, Assessment, Plan), BIRP (Behavior, Intervention, Response, Plan), or narrative format. SOAP notes are the most common progress note format because they provide a logical, standardized structure that works across all specialties and supports billing, audit compliance, and care continuity.
Can AI write SOAP notes automatically?
Yes. AI SOAP note generators like DeepCura use ambient listening technology to capture the patient encounter conversation and automatically structure it into a complete SOAP note with accurate Subjective, Objective, Assessment, and Plan sections. The AI identifies clinical information, maps it to the correct sections, suggests ICD-10 codes, and generates a draft that the provider reviews and approves before it is pushed to the EHR. This reduces documentation time from 10-15 minutes per note to approximately 30 seconds of review time.
How long should a SOAP note be?
SOAP note length depends on encounter complexity, not a word count target. A straightforward follow-up visit for a stable chronic condition may require a concise one-page note. A complex new patient evaluation with multiple problems, extensive workup, and detailed treatment plan may span two to three pages. The key is that every section contains enough detail to support your clinical reasoning and the E/M code billed, without unnecessary filler. A well-written SOAP note is complete, not long.
What are the most common SOAP note mistakes?
The most common mistakes include mixing Subjective and Objective data, writing an Assessment without clinical reasoning, using vague Plan items like "follow up as needed," copy-forwarding from previous notes without updating current findings, underdocumenting medical decision-making (which leads to downcoding), omitting pertinent negative findings, not documenting patient education, and signing notes days after the encounter. Each of these creates audit risk, reduces reimbursement, or compromises continuity of care.
Do therapists use SOAP notes?
Yes. SOAP notes are widely used in mental health settings by psychologists, licensed clinical social workers (LCSWs), licensed professional counselors (LPCs), and marriage and family therapists (MFTs). The Subjective section captures the client's reported mood, stressors, and progress. The Objective section documents the mental status exam, screening scores (PHQ-9, GAD-7), and behavioral observations. The Assessment states the diagnosis with treatment progress. The Plan outlines therapy interventions, homework, medication coordination, and next session scheduling. Some therapists prefer DAP or BIRP formats, but SOAP remains the most recognized and widely accepted.
Is there a free SOAP note template I can use?
Yes — all 10 SOAP note templates in this guide are free to use and copy. They cover primary care, mental health, physical therapy, pediatrics, dermatology, orthopedics, emergency medicine, neurology, cardiology, and chiropractic. Each template includes the complete S-O-A-P structure with placeholder fields you can replace with patient-specific information. For a fully automated solution that eliminates templates entirely, AI SOAP note generators like DeepCura create specialty-specific notes from the encounter conversation in real time.
Final Thoughts
SOAP notes are the backbone of clinical documentation — and they do not have to be the time sink that drains your day. The 10 templates and 6 real-world examples in this guide give you a ready-made framework for every major specialty, from primary care sick visits to emergency department chest pain workups.
The format itself is simple: what the patient told you (S), what you found (O), what you think (A), and what you are going to do about it (P). Getting each section right — with specific data, clinical reasoning, and actionable plans — is what separates a note that survives an audit from one that gets flagged.
For clinicians who want to move beyond templates entirely, AI SOAP note generators represent the most significant documentation advancement since the EHR itself. Instead of filling in brackets after every encounter, the AI listens, structures, and drafts — and you review and approve. The 10-15 minutes per note becomes 30 seconds. Multiplied across a full patient panel, that is hours returned to patient care or personal time every day.
For more clinical documentation guides, explore our biopsychosocial assessment template, doctor's note template, and patient intake form guide. For specialty-specific AI scribe recommendations, see our guides for psychiatry, physical therapy, dermatology, and emergency medicine. If you are ready to stop writing SOAP notes manually, try DeepCura free — no credit card required.
References
[1] Weed, L.L., "Medical Records, Medical Education, and Patient Care," Press of Case Western Reserve University, 1969.
[2] American Medical Association, "Current Procedural Terminology (CPT) — Evaluation and Management Services Guidelines," AMA. ama-assn.org/practice-management/cpt
[3] Centers for Medicare & Medicaid Services, "ICD-10-CM Official Guidelines for Coding and Reporting," CMS.gov. cms.gov/medicare/coding-billing/icd-10-codes
[4] U.S. Department of Health and Human Services, "HIPAA for Professionals — Privacy Rule," HHS.gov. hhs.gov/hipaa/for-professionals/privacy
[5] American Health Information Management Association, "Documentation Requirements for the Patient Medical Record," AHIMA. ahima.org
[6] Centers for Medicare & Medicaid Services, "Evaluation and Management (E/M) Visit Frequently Asked Questions," CMS.gov. cms.gov/medicare/payment/fee-for-service-payment/evaluation-management-services
[7] American Psychological Association, "Record Keeping Guidelines," APA. apa.org/practice/guidelines/record-keeping
[8] American Physical Therapy Association, "Documentation Authority for Physical Therapy Services," APTA. apta.org
[9] Centers for Medicare & Medicaid Services, "ICD-10-CM Official Coding Guidelines," CMS.gov. cms.gov/medicare/coding-billing/icd-10-codes/icd-10-cm-official-guidelines-coding-reporting
[10] World Health Organization, "International Classification of Diseases (ICD)," WHO. who.int/classifications/icd
[10] Office of the National Coordinator for Health Information Technology, "What is an Electronic Health Record (EHR)?," HealthIT.gov. healthit.gov/faq/what-electronic-health-record-ehr