Internists working in inpatient hospitalist, outpatient ambulatory, and consult-liaison settings produce some of the most documentation-heavy clinical notes in medicine — a typical hospitalist H&P runs 4-7 pages with full ROS across 14 systems, comprehensive past medical history with active problem list reconciliation, complete medication reconciliation against home, admission, transfer, and discharge medication lists, full social history with substance use details, code status documentation with POLST/MOST/MOLST review, ECOG performance status, comprehensive physical exam, problem-based assessment with differential diagnosis ranked by probability, and detailed multi-problem plan with GDMT (guideline-directed medical therapy) for each chronic condition. Outpatient internal medicine encounters carry comparable depth across longitudinal chronic disease management — diabetes (HbA1c targets, GLP-1 vs SGLT2 selection), hypertension (JNC-8 / ACC-AHA targets, ACE/ARB/CCB/thiazide selection), heart failure (GDMT pillars: ACEI/ARB/ARNI + beta-blocker + MRA + SGLT2i), atrial fibrillation (CHA2DS2-VASc/HAS-BLED, DOAC selection), CKD (KDIGO staging, nephrology referral triggers), CAD (secondary prevention bundle), COPD (GOLD ABE classification), and polypharmacy management with Beers Criteria deprescribing in older adults.
We ranked 6 AI scribes on the criteria that matter most for internal medicine documentation:
- Hospitalist H&P, progress note, and discharge summary depth — does the AI produce the comprehensive H&P with full ROS, problem-based A&P, and the structured progress note (HPI update, interval events, exam, labs/imaging, problem-based assessment) that hospitalists need?
- GDMT documentation with guideline citation — does it document guideline-directed therapy for HF (ACEI/ARB/ARNI + BB + MRA + SGLT2i with target doses), AFib (CHA2DS2-VASc score and DOAC selection), CKD (KDIGO stage and ACE/ARB/SGLT2i), diabetes (ADA Standards of Care 2026 with GLP-1/SGLT2 indications), and CAD (high-intensity statin, ASA, beta-blocker, ACE/ARB)?
- Code status, POLST, and goals-of-care capture — does it capture full code/DNR/DNI status, POLST/MOST/MOLST presence, healthcare proxy/POA, advance directive status, and goals-of-care conversation documentation?
- Beers Criteria, deprescribing, and polypharmacy management — does it flag Beers Criteria potentially inappropriate medications (PIMs) in older adults, support deprescribing reasoning, and document polypharmacy assessment?
All products were evaluated in February-April 2026. Pricing reflects publicly available rates. Internal medicine practices range from solo outpatient to hospitalist groups embedded in academic medical centers — integration depth and feature requirements vary meaningfully across these settings.
Disclosure & methodology. This comparison is published by DeepCura, which is included in the ranking. Pricing and feature claims for competitor products reflect publicly available information as of the evaluation period above and may change — verify directly with each vendor before procurement. This article is editorial commentary; it is not medical, legal, billing, or compliance advice. CPT® is a registered trademark of the American Medical Association. ACC, AHA, HFSA, USPSTF, AGS, ATS, IDSA, and other organization names referenced are trademarks of their respective owners; DeepCura is not affiliated with or endorsed by these organizations. References are nominative and used for descriptive comparison only.
Why Internal Medicine Needs an AI Scribe
The Documentation Reality in Internal Medicine
Internal medicine is one of the broadest documentation-burden specialties because it spans:
- Hospital medicine (hospitalist) — H&P at admission (4-7 pages), daily progress notes (1-3 pages each, often 8-15 patients per day), consult notes when serving as PCP-of-record, transfer summaries, discharge summaries (2-5 pages with detailed medication reconciliation, follow-up coordination, and primary care handoff)
- Outpatient ambulatory — comprehensive new patient intakes (often 60 minutes for complex multi-comorbidity patients), follow-up visits with chronic disease management (HF, AFib, CKD, diabetes, hypertension, CAD, COPD, dementia), preventive care (USPSTF screenings, immunizations), Medicare AWV (G0438 initial / G0439 subsequent), Transitional Care Management (99495/99496), Chronic Care Management (99490/99437/99491/99487/99489), Principal Care Management (99424-99427)
- Consult-liaison and subspecialty co-management — when an internist is consulted by surgical or specialty services for perioperative medical management, when comanaging complex multi-organ patients
- Procedural internal medicine — for those performing in-office procedures (joint injections, IUD placement, skin biopsies, treadmill stress, EKG interpretation, spirometry interpretation)
Across these settings, an internist generates 8-25 documentation products per day with varying depth. A hospitalist on a typical 12-hour shift writes one H&P, 8-12 progress notes, often 1-2 discharge summaries, and various order sets — easily 4-6 hours of documentation work compressed into a 12-hour shift alongside rounding, family meetings, procedures, and code response. Sinsky et al. (2016) documented physicians spend 49% of office hours on EHR work and desk work, with internal medicine cited among the highest-burden specialties.
What General-Purpose AI Scribes Miss in Internal Medicine
Most AI medical scribes are tuned for the 15-minute outpatient encounter — HPI, focused exam, MDM, plan. Internal medicine documentation breaks general-purpose scribes in specific ways:
- The hospitalist H&P is not an outpatient note. A hospitalist H&P includes a full 14-system ROS, complete past medical history with active problem reconciliation, full medication reconciliation (home meds vs ED-administered vs admission orders with discrepancy reconciliation), comprehensive social history including alcohol and substance use, code status with POLST/MOST/MOLST review, healthcare proxy and POA review, advance directive review, ECOG performance status (0-5), Karnofsky if oncology-relevant, frailty assessment in older adults, full physical exam with pertinent positives and negatives, problem-based assessment with differential ranked by probability and supporting evidence, and a detailed problem-based plan with GDMT for each chronic condition.
- Problem-based assessment and plan, not narrative. Internal medicine note structure organizes A&P by problem (often as a numbered list — #1 Acute decompensated HF, #2 AFib with RVR, #3 CKD stage 3b, #4 T2DM, #5 HTN, #6 Hyperlipidemia, #7 OSA, #8 GERD), with each problem getting its own assessment paragraph and plan items. A scribe that produces a single combined assessment narrative loses the structure essential to internal medicine cognition.
- GDMT for chronic disease management. ADA Standards of Care 2026 for diabetes (HbA1c target individualized 6.5%-8.0% by life expectancy and complications, GLP-1 RA with cardiovascular benefit indications, SGLT2i with HF/CKD indications, semaglutide oral and injectable, tirzepatide), 2022 ACC/AHA/HFSA HF Guideline with 2024 focused update (ACEI/ARB/ARNI + evidence-based BB + MRA + SGLT2i pillars with target doses), 2023 ACC/AHA Guideline for AFib (CHA2DS2-VASc with sex-specific scoring, HAS-BLED, DOAC selection by GFR), KDIGO 2024 CKD guideline (stage by GFR + albuminuria with risk categorization), 2018 ACC/AHA Cholesterol Guideline (high-intensity statin in ASCVD, primary prevention thresholds), GOLD 2026 COPD (ABE classification, LABA/LAMA/ICS step-up). The AI must document what therapy is initiated, what dose, what target, and what guideline supports it.
- Beers Criteria and deprescribing. AGS Beers Criteria 2023 update flags potentially inappropriate medications (PIMs) in older adults — anticholinergics (diphenhydramine, oxybutynin), benzodiazepines (alprazolam, lorazepam, clonazepam — all flagged in older adults due to fall and cognitive risk), proton pump inhibitors (long-term use beyond 8 weeks without indication), NSAIDs (chronic use in CKD, HF, on anticoagulation), digoxin >0.125mg/day, spironolactone >25mg/day in CKD, glyburide (sulfonylurea with high hypoglycemia risk in older adults), zolpidem (extended use). The AI should flag PIMs and support deprescribing documentation.
- Polypharmacy and medication reconciliation. Hospital admission requires reconciliation of home medications against admission orders — what is continued, modified, held, or discontinued and why. Hospital discharge requires reconciliation of admission medications against discharge plan with explicit rationale for each change communicated to patient and PCP.
- Code status and goals-of-care documentation. Full code, DNR, DNI, comfort care, and limited-trial status with POLST/MOST/MOLST review and update. Goals-of-care conversations require documentation of the conversation participants, the patient or surrogate decision-maker preferences, the prognosis communication, and the resulting plan. CMS reimburses Advance Care Planning (99497/99498) when documented appropriately.
- Quality measure documentation. HEDIS measures (HbA1c control, blood pressure control, statin therapy in diabetes, eye exam, nephropathy screening), CMS Stars measures, MIPS quality measures, and value-based-care metrics that affect both primary care contracts and ACO performance. Internal medicine practices in capitated arrangements have direct revenue tied to documentation completeness.
- Transitional Care Management and Chronic Care Management coding. TCM (99495 moderate complexity / 99496 high complexity) requires documentation of post-discharge interactive contact within 2 business days, comprehensive medication reconciliation, and face-to-face visit within 7 days (high complexity) or 14 days (moderate). CCM (99490 first 20 minutes / 99437 next 20 minutes / 99491 physician-only first 30 minutes / 99487 first 60 minutes complex / 99489 each additional 30 minutes complex) requires documented care plan, consent, 24/7 access, and time tracking. PCM (99424-99427) for single-condition focus.
- Subspecialty-aware differential generation. Internal medicine differential includes specialty-aware reasoning — the dyspneic patient differential includes cardiac (HF, ischemia, arrhythmia, pericardial), pulmonary (PE, pneumonia, COPD exacerbation, asthma exacerbation, pleural effusion), and other (anemia, anxiety, deconditioning) — and the AI should support breadth-and-depth differential thinking.
Audit, Quality, and Reimbursement Stakes
Internal medicine documentation has direct quality and reimbursement consequences. Inpatient documentation drives DRG assignment and severity-of-illness/risk-of-mortality (SOI/ROM) coding which determines hospital payment. Outpatient documentation drives RVU capture, HEDIS performance, ACO quality scores, and value-based-care payments. CDI (Clinical Documentation Improvement) programs aggressively review hospitalist documentation for missed CC/MCC capture (e.g., acute systolic HF instead of just HF, sepsis with organ dysfunction instead of just infection, acute kidney injury with stage instead of just AKI).
The OIG and CMS audit internal medicine claims for E&M level support, time-based coding documentation (post-2021 E&M revision), and chronic care management compliance. PE quality measures (5-component bundle), sepsis bundles, AMI bundles, HF bundles all have documentation requirements that affect both quality scores and value-based-purchasing.
An AI scribe that supports the hospitalist H&P depth, problem-based A&P structure, GDMT documentation with guideline citation, Beers Criteria flagging, and polypharmacy reconciliation directly affects both audit defensibility and revenue capture for internal medicine practices.
Quick Comparison — Top AI Scribes for Internal Medicine
| Rank | Tool | Price | IM-Specific | EHR Integration | Best For |
|---|---|---|---|---|---|
| 1 | DeepCura | $129/mo | Custom hospitalist + ambulatory + GDMT templates | 9 EHRs (custom mapping) | Best Overall |
| 2 | Abridge AI | Custom enterprise | Hospitalist enterprise focus | Epic deep | Hospitalist systems |
| 3 | Nuance DAX Copilot | Custom enterprise | Enterprise EHR-native | Epic, Cerner deep | Epic/Cerner shops |
| 4 | Freed AI | $39-$104/mo | Generic outpatient SOAP | Browser scrape (Premier) | Outpatient solo |
| 5 | DeepScribe | ~$199/mo | Customizable templates | Custom builds | Customization |
| 6 | Heidi Health | $0-$99/mo | Generic templates, IM-adaptable | Limited write-back | Free tier trial |
For a broader cross-specialty comparison, see our Best AI Medical Scribes in 2026 ranking. For family medicine and primary care tool selection, see our best AI scribe for family medicine guide.
What to Look For in an Internal Medicine AI Scribe
Internal medicine documentation requires depth that outpatient-only AI scribes don't deliver. Before choosing a tool, evaluate it against these eight criteria:
1. Hospitalist H&P, Progress Note, and Discharge Summary Templates. The AI must produce comprehensive H&P with 14-system ROS, problem-based A&P, complete medication reconciliation; progress notes with HPI update, interval events, exam, labs/imaging, problem-based assessment; and discharge summaries with medication reconciliation, follow-up coordination, and PCP handoff.
2. Problem-Based Assessment and Plan Structure. Numbered or bulleted problem list with each problem getting an assessment paragraph and plan items. Not a single combined narrative.
3. GDMT with Guideline Citation. Documentation that not only states the medication initiated but cites the supporting guideline (ADA Standards of Care 2026 for diabetes, 2022 ACC/AHA/HFSA HF Guideline with 2024 focused update, 2023 ACC/AHA Guideline for AFib, KDIGO 2024 for CKD, 2018 ACC/AHA Cholesterol Guideline, GOLD 2026 for COPD).
4. Beers Criteria Flagging. AGS Beers Criteria 2023 PIMs flagged in older adults with deprescribing reasoning support.
5. Code Status and Goals-of-Care Documentation. Full code/DNR/DNI status, POLST/MOST/MOLST review and update, healthcare proxy and POA review, advance directive review, ACP conversation documentation supporting 99497/99498 billing.
6. TCM, CCM, and PCM Time Tracking. TCM (99495/99496) post-discharge interactive contact within 2 business days, medication reconciliation, and face-to-face visit timing. CCM (99490/99437/99491/99487/99489) and PCM (99424-99427) time tracking for billing compliance.
7. Quality Measure Capture. HEDIS, CMS Stars, MIPS quality, ACO quality measure capture in the documentation flow rather than as a separate workflow.
8. EHR Integration with Inpatient and Ambulatory Workflows. Bidirectional integration with Epic (Hyperdrive), Cerner (Oracle Health), MEDITECH, athenahealth, eClinicalWorks. Hospitalists need integration that works with the inpatient EHR workflow including the hospital problem list, medication reconciliation tools, and order sets.
Detailed Reviews
1. DeepCura — Best Overall for Internal Medicine Documentation
DeepCura is a customizable clinical AI platform that combines ambient scribing, clinical decision support, evidence search, practice automation, and bidirectional EHR integration — $129/month with unlimited notes. For internal medicine — outpatient ambulatory practices, hospitalist groups outside the largest academic systems, and integrated primary care + hospital medicine practices — DeepCura's customizable templates and unlimited per-user notes deliver the strongest fit because internal medicine documentation depth requires structural support that no off-the-shelf scribe ships with by default.
For internists, the key differentiator is template flexibility across the breadth of internal medicine settings. DeepCura's custom template builder lets practice leads encode setting-specific templates: a hospitalist H&P template with chief complaint, full HPI, complete past medical/surgical/social/family history, allergies, full medication reconciliation (home vs admission with discrepancy notes), full ROS across 14 systems, comprehensive physical exam, results review, problem-based assessment with differential ranking, and detailed problem-based plan with GDMT for each chronic condition; a hospitalist progress note template with HPI update, interval events, vital trend, I&O if relevant, exam, labs/imaging, problem-based assessment update, and plan changes; a discharge summary template with admit/discharge dates, principal diagnosis, secondary diagnoses, hospital course narrative, complete medication reconciliation with rationale for changes, condition at discharge, follow-up coordination, and PCP handoff; an outpatient comprehensive new patient template with full preventive care review (USPSTF screenings, immunizations), chronic disease management for each comorbidity, and care planning; an outpatient follow-up template with problem-based update; AWV templates (G0438/G0439); TCM templates with day-of-discharge contact and 7/14-day visit; CCM/PCM time tracking templates; ACP templates supporting 99497/99498.
CDS Mode (3 credits per encounter) generates clinical decision support — particularly valuable for the multi-system inpatient where dyspnea differential includes cardiac/pulmonary/embolic/anemic/anxiety; for goals-of-care conversations in advanced disease where prognosis communication and treatment alignment require careful framing; and for medication reconciliation in older adults where Beers Criteria and renal/hepatic dosing concerns intersect.
DeepEvidentia — DeepCura's evidence search engine — surfaces references and excerpts from publicly indexed sources including PubMed/MEDLINE, Cochrane, ACC/AHA guidelines, ADA Standards of Care, KDIGO guidelines, GOLD reports, USPSTF recommendations, Choosing Wisely lists, AGS Beers Criteria, and CMS coverage determinations. Useful for internists practicing across the breadth of internal medicine where evidence access at the bedside or visit reduces friction in clinical decision-making.
Strengths:
- Custom templates per setting (hospitalist H&P, progress, discharge; outpatient comprehensive, follow-up; AWV; TCM; CCM/PCM; ACP) with internal medicine conventions
- GDMT documentation with guideline citation across HF, AFib, CKD, diabetes, CAD, COPD
- Beers Criteria flagging in older adults
- Polypharmacy and medication reconciliation support
- Code status and goals-of-care documentation
- Quality measure capture (HEDIS, CMS Stars, MIPS, ACO)
- AI receptionist for after-hours triage and intake — particularly valuable for outpatient internal medicine practices
- Multiple AI engines matched to documentation complexity (1-15 credits)
- Unlimited notes per provider on all plans
- Bidirectional integration with Epic, Cerner, athenahealth, AdvancedMD, eClinicalWorks via custom field mapping
Limitations:
- Custom template builder requires meaningful initial setup (15-25 hours per practice to encode hospitalist + ambulatory + chronic disease management templates)
- Native Epic Hyperdrive integration depth is via API/mapping rather than out-of-box; large hospitalist groups in Epic-native environments may prefer Abridge or DAX Copilot for path-of-least-resistance procurement
- Real-time inpatient context (live labs, vitals, medication administration data) integration requires verifying setup with the hospital's EHR team
Pricing: $129/month per provider — all features included. Free trial available, no credit card required.
Verdict: DeepCura is the strongest choice for internal medicine practices outside the largest enterprise health systems — independent outpatient internists, small to mid-scale hospitalist groups, integrated primary care + hospital medicine practices, and group practices in mixed inpatient/outpatient settings. The flexibility cost is upfront setup time, but the per-user pricing and unlimited notes make it economically viable at solo and group scale.
DeepCura: Customizable AI Scribe for Internal Medicine
Hospitalist H&P, progress, and discharge templates with GDMT documentation, Beers Criteria flagging, code status capture, and unlimited notes — $129/mo. Start your free trial.
+1 (415) 549-1829Available 24/7 · Set up in seconds · No credit card required
2. Abridge AI — Best for Hospitalist Systems
Abridge has emerged as the leading enterprise AI scribe for large health systems, with deployments at multiple major academic medical centers. The product is sold via custom enterprise contracts and supports hospitalist workflows with deep Epic Hyperdrive integration. For hospitalist groups embedded in academic medical centers and large health systems on Epic, Abridge offers consistent infrastructure across the medicine service and the broader clinical team.
The limitation is access — Abridge is enterprise-only and not available to small hospitalist groups, ambulatory internal medicine practices, or independent internists. Pricing is custom (per-provider per-month with multi-year contracts).
Pricing: Custom enterprise contracts. Multi-year minimum.
Verdict: Best for hospitalist groups embedded in large health systems with enterprise procurement and Epic deep integration requirements. Read our Abridge AI review.
3. Nuance DAX Copilot — Best for Deep Epic/Cerner Integration
Nuance DAX Copilot (Microsoft) is an incumbent enterprise AI scribe with extensive Epic and Cerner integration capabilities. DAX Copilot supports hospitalist and ambulatory internal medicine workflows in health-system contexts and integrates ambient documentation into Epic Hyperdrive and Cerner workflows.
For health systems already on Microsoft enterprise contracts (M365, Azure, Teams), DAX Copilot is the path-of-least-procurement-resistance and offers consistent infrastructure across roles including internal medicine.
The limitations parallel Abridge: enterprise-only, multi-year contracts, custom implementation. Not accessible to small ambulatory internal medicine practices or smaller hospitalist groups.
Pricing: Custom enterprise. Multi-year contracts.
Verdict: Best for health systems on Microsoft enterprise contracts with Epic or Cerner deep integration requirements.
4. Freed AI — Best for Outpatient Solo Internist
Freed AI is the most accessible ambient scribe for outpatient solo internal medicine practitioners. The product is built around the conventional outpatient encounter and produces SOAP-format notes by default. For outpatient internists running 15-25 visits per day, Freed at $79-$104/month with unlimited notes is one of the most cost-effective ambient scribes on the market.
Limitations for inpatient internal medicine: Freed is not designed for hospitalist H&P depth, multi-problem A&P structure, or hospital workflow integration. The Premier tier ICD-10 coding suggestion is helpful for outpatient chronic disease coding (E11.x diabetes, I10 hypertension, I50.x heart failure, I48.x AFib, N18.x CKD) but is not built for hospitalist documentation depth, CDI workflows, or DRG-aware narrative requirements (final code assignment is performed by certified coders/CDI specialists, not the AI scribe).
Pricing: $39/month (Starter, 40 notes), $79/month (Core, unlimited), $104/month (Premier, unlimited + EHR push + ICD-10).
Verdict: Best for outpatient solo internists who want fast ambient capture at the lowest defensible price point. Not the right fit for hospitalists or hospital-employed internists. Read our Freed AI review.
5. DeepScribe — Best for Customizable Internal Medicine Templates
DeepScribe offers customizable AI scribe templates with deeper specialty configuration than off-the-shelf consumer-grade tools. For internal medicine practices with internal template-building resources and willingness to invest in custom configuration, DeepScribe can produce hospitalist H&P-depth documentation, problem-based A&P, and GDMT-aware notes.
Trade-off is price — DeepScribe is approximately $199/month per provider, roughly 50% higher than DeepCura at the same custom-template tier. DeepScribe also lacks DeepCura's bundled CDS, evidence search, and AI receptionist features.
Pricing: Approximately $199/month per provider.
Verdict: Best for internal medicine practices willing to pay a premium for custom-template ambient capture without the broader DeepCura platform features. Read our DeepScribe review.
6. Heidi Health — Best Free Tier for Internist Trial
Heidi Health offers a usable free tier (limited notes per month) that lets individual internists test ambient AI documentation at zero cost. Heidi has multi-specialty templates available and adapts to internal medicine workflows with custom configuration.
US internal medicine conventions (hospitalist H&P depth, problem-based A&P, US-specific quality measures, Medicare AWV/TCM/CCM coding) require manual configuration on Heidi. PMS integration is limited (clipboard or email).
Pricing: Free tier (limited notes), Pro tier roughly $129/month, enterprise tier higher.
Verdict: Best for individual outpatient internists who want to test ambient AI documentation at zero cost before committing to a paid tool. Read our Heidi Health review.
Head-to-Head — Internal Medicine Documentation Features
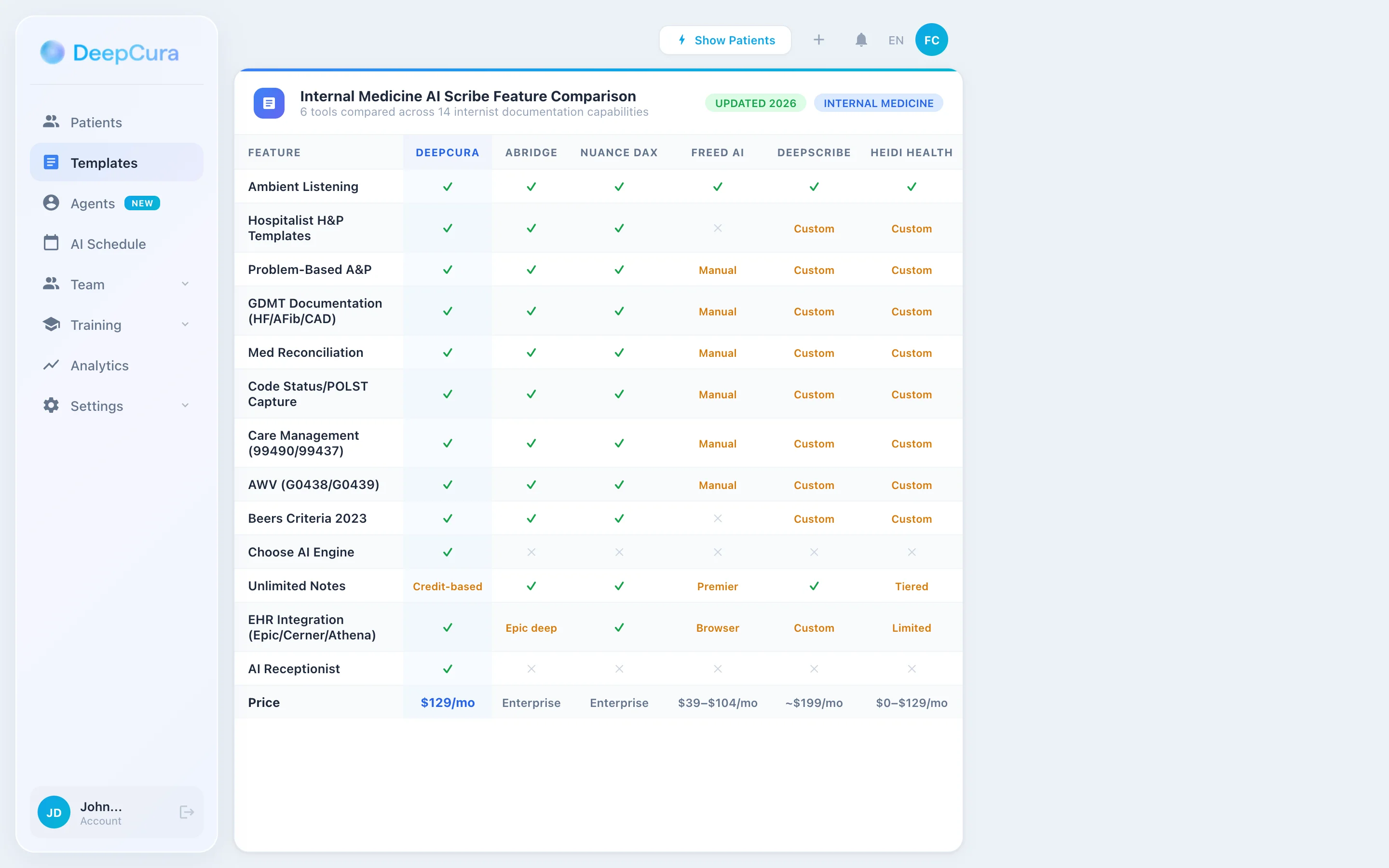
| Feature | DeepCura | Abridge | Nuance DAX | Freed | DeepScribe | Heidi |
|---|---|---|---|---|---|---|
| Hospitalist H&P Template | ✓ Custom | ✓ Enterprise | ✓ Enterprise | ✗ | ✓ Custom | Custom |
| Problem-Based A&P Structure | ✓ | ✓ | ✓ | Manual | ✓ Custom | Custom |
| GDMT Documentation (HF/AFib/CKD/DM/CAD/COPD) | ✓ | ✓ | ✓ | Manual | ✓ Custom | Custom |
| Beers Criteria Flagging | ✓ | ✓ | ✓ | ✗ | Custom | Custom |
| Code Status / POLST / Goals-of-Care | ✓ | ✓ | ✓ | Manual | ✓ Custom | Custom |
| Polypharmacy / Med Reconciliation | ✓ | ✓ | ✓ | Manual | ✓ Custom | Custom |
| AWV (G0438/G0439) | ✓ Custom | ✓ Enterprise | ✓ Enterprise | Manual | ✓ Custom | Custom |
| TCM (99495/99496) | ✓ Custom | ✓ Enterprise | ✓ Enterprise | Manual | ✓ Custom | Custom |
| CCM / PCM Time Tracking | ✓ Custom | ✓ Enterprise | ✓ Enterprise | Manual | ✓ Custom | Custom |
| ACP (99497/99498) | ✓ Custom | ✓ Enterprise | ✓ Enterprise | Manual | ✓ Custom | Custom |
| AI Receptionist (intake/triage) | ✓ | ✗ | ✗ | ✗ | ✗ | ✗ |
| Clinical Decision Support | ✓ (CDS Mode) | Limited | Limited | ✗ | Limited | ✗ |
| EHR Bidirectional | 9 EHRs | Epic deep | Epic/Cerner deep | Browser scrape | Custom builds | Limited |
| Price | $129/mo all features | Enterprise custom | Enterprise custom | $39-$104/mo | ~$199/mo | $0-$99/mo |
Internal Medicine Workflow with DeepCura
DeepCura's tiered credit system lets internists match AI resources to documentation complexity — fast for routine follow-ups, deeper for hospitalist H&Ps and complex multi-problem cases.
Routine Outpatient Follow-Up (1 Credit) — Established Patient Chronic Disease Visit
For 15-20 minute outpatient follow-up — chronic disease management with HbA1c review, BP review, medication adjustment, screening review, and brief plan — the 1-credit model generates a complete problem-based note in under 30 seconds. Speed-optimized for the outpatient internist running 18-25 visits per day where efficient documentation completion preserves cognitive bandwidth.
Comprehensive Visit and Goals-of-Care (3 Credits CDS) — AWV, TCM, ACP, Complex Multi-Comorbidity
For Annual Wellness Visits with full preventive care review and screening update; Transitional Care Management visits with hospital course review, medication reconciliation, and follow-up coordination; Advance Care Planning conversations with prognosis communication, healthcare proxy review, and treatment preference documentation; complex multi-comorbidity outpatient visits with 5+ active problems requiring coordinated management — CDS Mode generates the structured comprehensive narrative with appropriate billing code support.
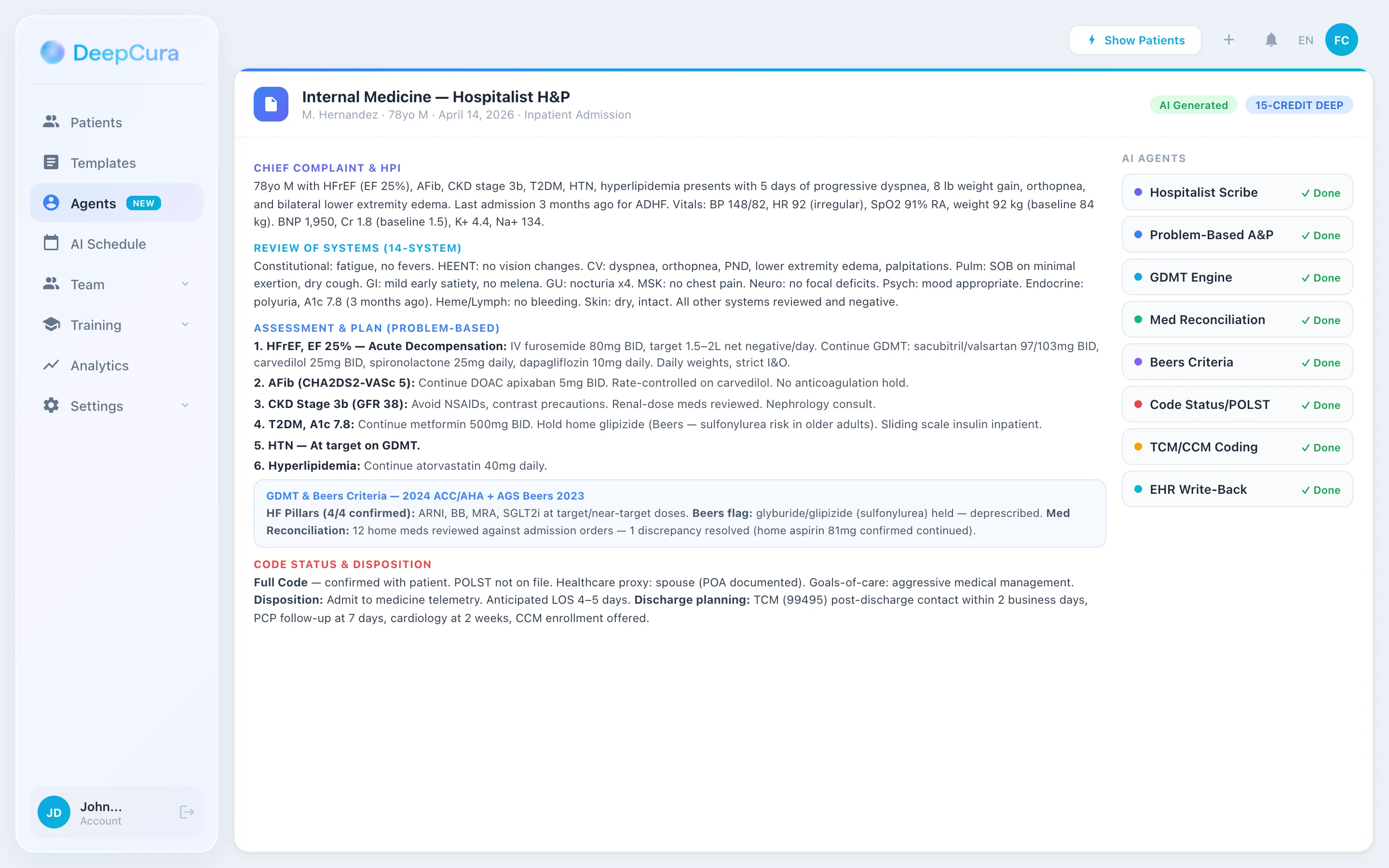
Hospitalist H&P and Discharge (15 Credits) — Inpatient Admission, Complex Discharge
For hospitalist H&P at admission with full ROS across 14 systems, complete medication reconciliation, code status review, and detailed problem-based assessment and plan; for complex discharge summaries with detailed hospital course, medication reconciliation with rationale for changes, follow-up coordination, and PCP handoff — the maximum-depth model produces a comprehensive narrative intended to support documentation completeness for downstream CDI review and continuity of care (final coding and DRG assignment are performed by certified coders/CDI staff).
From Bedside Round to Documentation in Real Time
DeepCura templates for hospitalist H&P, progress, discharge, AWV, TCM, CCM/PCM, and ACP with GDMT documentation, Beers Criteria flagging, and quality measure capture — $129/mo. Start your free trial.
+1 (415) 549-1829Available 24/7 · Set up in seconds · No credit card required
Clinical Decision Support and Evidence Search for Internists
CDS Mode outputs are documentation-aid suggestions for clinician review. They are not diagnoses, treatment recommendations, or substitutes for clinical judgment. The clinician retains full responsibility for diagnosis, workup, and treatment decisions. Drug names, doses, and regimens that may appear in examples are illustrative summaries of published guidelines and are not patient-specific recommendations. DeepCura is not an FDA-cleared medical device.
CDS Mode — Decision Support for Multi-System Internal Medicine Cases
Internists encounter multi-system presentations where differential diagnosis breadth and depth matter. CDS Mode provides decision support for:
- Multi-system differential generation — the dyspneic patient (cardiac: HF, ischemia, arrhythmia, pericardial; pulmonary: PE, pneumonia, COPD, asthma, pleural effusion, pulmonary HTN; other: anemia, anxiety, deconditioning), the AKI patient (pre-renal: hypovolemia, HF, hepatorenal, sepsis; intrinsic: ATN, AIN, GN, vascular; post-renal: BPH, stones, bladder outlet), the altered mental status patient (metabolic, infectious, neurologic, pharmacologic, psychiatric)
- GDMT optimization in HF — the patient with HFrEF on partial GDMT (e.g., on ACEI but not ARNI, on BB but not titrated to target, no MRA, no SGLT2i) — CDS Mode flags GDMT gaps and titration opportunities aligned to ACC/AHA guidelines
- Goals-of-care reasoning in advanced disease — when does conservative management vs aggressive management align with patient values? When is hospice referral indicated? When is palliative care consultation appropriate?
- Polypharmacy and Beers Criteria reasoning — older adult on 12 medications with cognitive impairment — what to deprescribe and how
- Inpatient sepsis and shock differentiation — septic vs cardiogenic vs hypovolemic vs distributive shock differential
For an admission encounter with HFrEF features (reduced ejection fraction, elevated BNP, and decompensation findings), CDS Mode can surface documentation prompts derived from the 2022 ACC/AHA/HFSA Heart Failure Guideline (and the 2023 focused update): differential considerations to document and rule out (acute decompensated HF, pulmonary embolism, ischemia, AFib), four-pillar GDMT categories the chart should explicitly address (ACEI/ARB/ARNI, evidence-based beta-blockers, MRAs, and SGLT2 inhibitors — with stated contraindications when omitted), Beers Criteria considerations to flag if relevant medications are added, and goals-of-care prompts (code status, palliative care). All clinical decisions — including whether to add, hold, or titrate any medication — are made by the treating clinician based on the full clinical picture; CDS Mode is a documentation aid, not a treatment recommendation engine.
DeepEvidentia — Evidence at the Bedside and Visit for Internists
DeepEvidentia provides real-time access to PubMed, Cochrane, NEJM, JAMA, Annals of Internal Medicine, ACP Annals, ACC/AHA guidelines, ADA Standards of Care, KDIGO guidelines, GOLD reports, USPSTF recommendations, Choosing Wisely, AGS Beers Criteria, and CMS coverage determinations.
Example queries internists actually ask:
- "GDMT for HFrEF — four pillars per 2022 ACC/AHA/HFSA HF guideline (and 2023 focused update)" — returns the four guideline-recommended pharmacologic categories (ACEI/ARB/ARNI, evidence-based beta-blockers, MRAs, SGLT2 inhibitors) with citation excerpts; specific drug selection, dose, and titration are clinician decisions made against the patient's clinical context, contraindications, and labs
- "DOAC selection in AFib by GFR" — returns CrCl-based dosing for apixaban, rivaroxaban, dabigatran, edoxaban with CrCl
<15considerations (apixaban often preferred) - "Beers Criteria 2023 — benzodiazepines in older adults" — returns AGS recommendation against benzodiazepine initiation and the deprescribing rationale
- "Sepsis 3 criteria and qSOFA" — returns the Sepsis 3 definition and qSOFA threshold (≥2 of altered mental status, RR ≥22, SBP ≤100)
- "USPSTF colorectal cancer screening 2021 update" — returns the age 45-75 screening start with options
- "ACP guideline on chronic insomnia management" — returns the CBT-I first-line recommendation
- "Choosing Wisely — imaging in low back pain" — returns the recommendation against imaging in non-specific low back pain without red flags
For internists practicing across the breadth of internal medicine, evidence access at the visit and bedside reduces friction in clinical decision-making.
Pricing Comparison
| Tool | Monthly | Note Limit | IM-Specific | Best Plan |
|---|---|---|---|---|
| DeepCura | $129/mo | Unlimited | ✓ Custom hospitalist + ambulatory | Single plan, all features |
| Abridge AI | Enterprise custom | Enterprise | ✓ | Enterprise contract |
| Nuance DAX Copilot | Enterprise custom | Enterprise | ✓ | Enterprise contract |
| Freed AI | $39-$104/mo | 40-unlimited | Outpatient only | Premier ($104) |
| DeepScribe | ~$199/mo | Unlimited | ✓ Custom | Custom-built tier |
| Heidi Health | $0-$99/mo | Free tier limited | Custom | Free or Pro |
See DeepCura in Action
Watch how DeepCura handles the full internal medicine workflow — hospitalist H&P with full ROS, problem-based assessment and plan, GDMT documentation with guideline citation, Beers Criteria flagging, polypharmacy and medication reconciliation, code status and goals-of-care, and quality measure capture.

Frequently Asked Questions
What is the best AI scribe for internal medicine?
DeepCura is the strongest cross-functional choice for internal medicine practices outside the largest enterprise health systems — independent outpatient internists, small to mid-scale hospitalist groups, integrated primary care + hospital medicine practices, and group practices in mixed inpatient/outpatient settings. Customizable templates support hospitalist H&P, progress, discharge, AWV, TCM, CCM/PCM, ACP, and chronic disease management with GDMT documentation. For large hospitalist groups in academic medical centers on Epic, Abridge AI and Nuance DAX Copilot are the enterprise leaders.
Do AI scribes produce hospitalist-grade H&P with full ROS and problem-based A&P?
DeepCura supports custom hospitalist H&P templates with full 14-system ROS, complete past medical/surgical/social/family history, comprehensive medication reconciliation, code status and goals-of-care review, and problem-based assessment and plan with differential ranking. Enterprise tools (Abridge, Nuance DAX) support hospitalist documentation in their workflows. Outpatient-focused tools (Freed) are not designed for hospitalist H&P depth.
Can AI scribes document GDMT for HF, AFib, CKD, diabetes, and CAD with guideline citation?
DeepCura supports custom templates with GDMT documentation aligned to 2022 ACC/AHA/HFSA HF Guideline with 2024 focused update (ACEI/ARB/ARNI + BB + MRA + SGLT2i pillars with target doses), 2023 ACC/AHA AFib Guideline (CHA2DS2-VASc, HAS-BLED, DOAC selection by GFR), KDIGO 2024 CKD Guideline, ADA Standards of Care 2026, 2018 ACC/AHA Cholesterol Guideline, and GOLD 2026 COPD. Enterprise tools support GDMT documentation. Consumer scribes require manual addition of guideline citations.
Do AI scribes flag Beers Criteria potentially inappropriate medications in older adults?
DeepCura's templates can flag AGS Beers Criteria 2023 PIMs in older adults with deprescribing reasoning support — anticholinergics, benzodiazepines, long-term PPIs, NSAIDs in CKD/HF, glyburide, zolpidem, high-dose digoxin or spironolactone in CKD. Enterprise tools support Beers flagging. DeepEvidentia provides real-time Beers Criteria reference at the visit.
Can AI scribes capture code status, POLST, and goals-of-care documentation for ACP billing?
DeepCura's templates capture full code/DNR/DNI status, POLST/MOST/MOLST review, healthcare proxy and POA review, advance directive review, and ACP conversation documentation supporting CMS Advance Care Planning codes (99497 first 30 minutes, 99498 each additional 30 minutes). Enterprise tools support ACP documentation. Consumer scribes require manual structuring.
Do AI scribes support TCM (99495/99496), CCM (99490/99437/99491/99487/99489), and PCM (99424-99427) time tracking?
DeepCura's custom templates support TCM with post-discharge interactive contact within 2 business days documentation and face-to-face visit timing; CCM with 24/7 access, comprehensive care plan, and time tracking; and PCM single-condition focus documentation. Enterprise tools support these care management codes. Consumer scribes require manual time tracking.
Are AI scribes appropriate for hospitalist documentation completeness and CDI workflows?
DeepCura's hospitalist H&P templates and 15-credit deep narrative model are designed to support documentation completeness for CDI review — encouraging explicit acuity language (e.g., acute systolic HF rather than unspecified HF, sepsis with organ dysfunction, AKI with stage), comorbidity capture relevant to SOI/ROM, and the kind of specificity that CDI specialists and certified coders look for. Final code assignment and DRG determination are performed by certified coders/CDI staff, not the AI scribe. Enterprise tools (Abridge, Nuance DAX) are widely deployed in hospital systems for similar documentation-completeness use cases. Outpatient-focused consumer scribes are not designed for hospitalist documentation depth.
How much do AI scribes for internal medicine cost?
Solo-friendly outpatient options run $39-$130/month per provider (Freed $39-$104, Heidi Pro $99, DeepCura $129). DeepScribe is approximately $199/month. Enterprise tools (Abridge, Nuance DAX Copilot) for hospitalists are custom-priced with multi-year contracts. For most internal medicine practices outside the largest hospital systems, the $99-$130/month accessible-price tier with DeepCura provides extensive internal medicine-specific template support.
Final Verdict
For internal medicine practices, the choice comes down to four profiles:
Best overall: DeepCura at $129/month — customizable hospitalist H&P/progress/discharge templates, ambulatory comprehensive and follow-up templates, AWV (G0438/G0439), TCM (99495/99496), CCM (99490/99437/99491/99487/99489), PCM (99424-99427), ACP (99497/99498), GDMT documentation with guideline citation across HF/AFib/CKD/diabetes/CAD/COPD, Beers Criteria flagging, polypharmacy and medication reconciliation, code status and goals-of-care documentation, and quality measure capture (HEDIS, CMS Stars, MIPS, ACO). The strongest choice for internal medicine practices outside the largest enterprise health systems.
Best for hospitalist enterprise: Abridge AI and Nuance DAX Copilot — enterprise-grade with deep Epic and Cerner integration, multi-role/multi-specialty deployment, and the IT/security/legal frameworks that academic medical centers and large IDS/EDC organizations require. Custom enterprise pricing.
Best for outpatient solo: Freed AI Premier at $104/month — strong ambient capture quality with browser-based EHR push, suitable for outpatient solo internists who do not need hospitalist depth and are willing to work within outpatient-grade documentation defaults.
Best for free-tier internist trial: Heidi Health — free tier (limited notes) lets individual outpatient internists test ambient AI documentation at zero cost.
For a broader cross-specialty comparison, see our Best AI Medical Scribes in 2026 ranking. For family medicine and primary care tool selection, see our best AI scribe for family medicine and best AI scribe for medical professionals guides. For practices needing after-hours triage and intake automation, see our Best AI Medical Receptionist guide. For free copy-paste clinical templates, see our SOAP note template reference. If you are evaluating EMRs alongside the scribe decision, see our best EMR for small practices ranking.
References
[1] American College of Physicians, "ACP Annals of Internal Medicine Clinical Guidelines," ACP. acpjournals.org/journal/aim/category/clinical-guidelines
[2] Heidenreich PA, Bozkurt B, Aguilar D, et al., "2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure (and 2024 Focused Update)," Journal of the American College of Cardiology, 79(17), e263-e421, 2022. pubmed.ncbi.nlm.nih.gov/35379503
[3] Joglar JA, Chung MK, Armbruster AL, et al., "2023 ACC/AHA/ACCP/HRS Guideline for the Diagnosis and Management of Atrial Fibrillation," Circulation, 149(1), e1-e156, 2024. pubmed.ncbi.nlm.nih.gov/38033089
[4] Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group, "KDIGO 2024 Clinical Practice Guideline for the Evaluation and Management of CKD," Kidney International, 105(4S), S117-S314, 2024. kdigo.org/guidelines/ckd-evaluation-and-management
[5] American Diabetes Association, "Standards of Care in Diabetes 2026," Diabetes Care, 49(Suppl 1), 2026. diabetesjournals.org/care/issue/49/Supplement_1
[6] Grundy SM, Stone NJ, Bailey AL, et al., "2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol," Circulation, 139(25), e1082-e1143, 2019. pubmed.ncbi.nlm.nih.gov/30586774
[7] Global Initiative for Chronic Obstructive Lung Disease, "GOLD 2026 Report — Global Strategy for the Diagnosis, Management, and Prevention of COPD," GOLD. goldcopd.org
[8] American Geriatrics Society Beers Criteria Update Expert Panel, "American Geriatrics Society 2023 Updated AGS Beers Criteria for Potentially Inappropriate Medication Use in Older Adults," Journal of the American Geriatrics Society, 71(7), 2052-2081, 2023. pubmed.ncbi.nlm.nih.gov/37139824
[9] Sinsky C, Colligan L, Li L, et al., "Allocation of Physician Time in Ambulatory Practice: A Time and Motion Study in 4 Specialties," Annals of Internal Medicine, 165(11), 753-760, 2016. pubmed.ncbi.nlm.nih.gov/27595430
[10] Centers for Medicare & Medicaid Services, "Transitional Care Management, Chronic Care Management, Principal Care Management, and Advance Care Planning Service Codes," CMS. cms.gov/files/document/mln908628-care-management.pdf
[11] U.S. Preventive Services Task Force, "Final Recommendations — Screening Recommendations," USPSTF. uspreventiveservicestaskforce.org