Across the clinical care team — physicians, nurse practitioners, physician assistants, registered nurses, medical assistants, social workers, dietitians, and respiratory therapists — documentation is consistently the highest-cited driver of burnout, well above patient acuity, compensation, and call burden. The 2024 NAM (National Academy of Medicine) Clinician Well-Being Collaborative reported that interdisciplinary teams collectively spend more time on documentation than on direct patient care, with the after-hours "pajama time" charting load distributed unevenly across roles — physicians and APPs (advanced practice providers) carrying the heaviest individual burden, but RNs, MAs, and integrated allied health staff carrying meaningful documentation responsibilities that vary by setting (primary care, hospital, urgent care, post-acute, home health).
We ranked 6 AI scribes on the criteria that matter most for the full clinical care team:
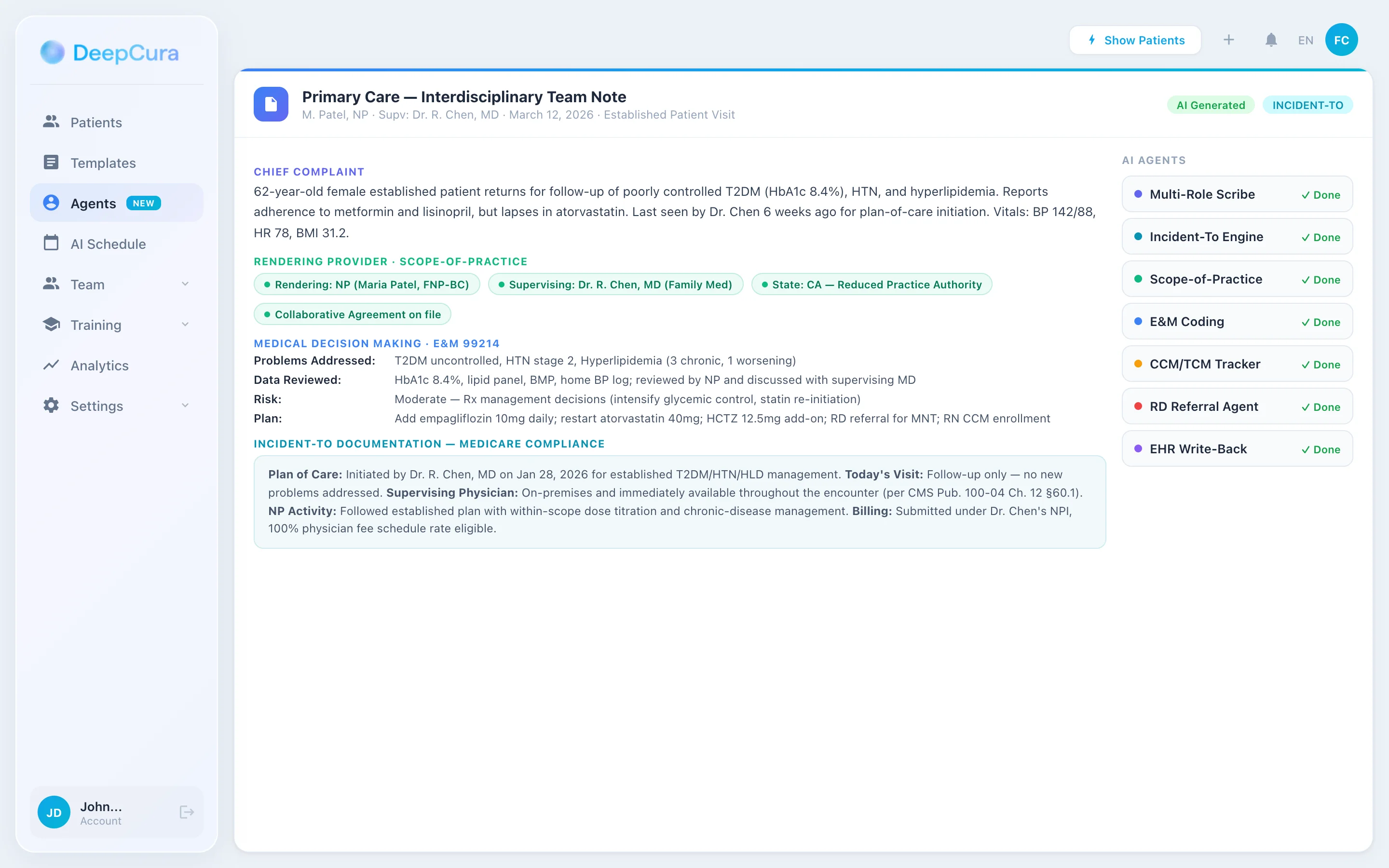
- Scope-of-practice and credentialing-aware documentation — does the AI tag the rendering provider correctly (MD, DO, NP, PA, RN, CNM, CRNA, MA, RD, MSW) and structure documentation to support each role's scope-of-practice and supervision/collaboration requirements?
- Incident-to and split/shared billing capture — does it support Medicare incident-to documentation (100% physician fee schedule rate when supervised vs. 85% APP direct billing) and CMS 2024 split/shared visit rules in hospital settings (substantive portion documentation)?
- Interdisciplinary team (IDT) documentation — does it support care plan documentation across team roles, transition-of-care notes (TCM 99495/99496), care management (CCM 99490/99487), and team-based care models including PCMH (Patient-Centered Medical Home) and ACO (Accountable Care Organization) requirements?
- Role-appropriate template depth — does it produce different note structures for an NP independent visit (full E&M MDM) vs. an MA intake summary vs. an RN care management call vs. an RD nutrition counseling note vs. an MSW SDoH screening note?
All products were evaluated in February-April 2026. Pricing reflects publicly available rates. Custom-priced products were assessed based on disclosed ranges and verified user reports.
Disclosure & methodology. This comparison is published by DeepCura, which is included in the ranking. Pricing and feature claims for competitor products reflect publicly available information as of the evaluation period above and may change — verify directly with each vendor before procurement. This article is editorial commentary; it is not medical, legal, billing, or compliance advice. CPT® is a registered trademark of the American Medical Association. All other product names and trademarks are property of their respective owners; references are nominative and do not imply affiliation or endorsement.
Why Medical Teams Need an AI Scribe
The Documentation Crisis Across Clinical Roles
Documentation burden is not unique to physicians. The 2024 NAM Clinician Well-Being Collaborative documented that across the clinical care team:
- Physicians (MD/DO) spend 5.9 hours of every clinical day on EHR documentation plus 1.77 hours of after-hours "pajama time" (Sinsky 2016, Arndt 2017 in primary care).
- Nurse Practitioners (NP) with full-practice authority report similar EHR time burdens to physicians, often higher in primary care because NPs disproportionately staff rural and underserved practices with shorter visit slots.
- Physician Assistants (PA) working in collaborative agreements average 4-5 hours daily on documentation and chart review.
- Registered Nurses (RN) in primary care and care management roles spend 35-40% of their time on documentation, including telephone triage notes, care plan updates, and population health outreach documentation.
- Medical Assistants (MA) spend 25-30% of their time on documentation — intake summaries, vitals, screening tools (PHQ-9, GAD-7, AUDIT, ACE), and EHR data entry that the physician/APP later builds upon.
- Registered Dietitians (RD), Behavioral Health Counselors / Social Workers (MSW/LCSW), Respiratory Therapists (RT), and Pharmacists (PharmD) in integrated care teams contribute their own documentation that must coexist with the physician/APP note in a coherent chart.
The result is a team-wide documentation tax that shifts work between roles depending on where the bottleneck is, but rarely reduces in aggregate. PCMH-recognized practices and ACO participants have explicit care-coordination documentation requirements that compound on top of routine encounter notes.
What General-Purpose AI Scribes Miss for the Full Care Team
Most AI medical scribes are designed for a single physician-patient encounter — typically a 15-minute primary care office visit. The clinical care team operates under different documentation conventions that break single-role scribes:
- Scope-of-practice variation by state and role. NP scope-of-practice ranges from full-practice authority (27 states, DC, and U.S. territories (Guam, Northern Mariana Islands) per AANP as of the evaluation period; verify current status with your state board of nursing) to reduced practice authority (collaborative agreement required for prescribing or some practice elements) to restricted practice authority (supervisory agreement required for most practice). PA scope-of-practice operates under collaborative agreements that vary by state and specialty. The AI must tag the rendering provider correctly because the documentation conventions and billing rules differ by role.
- Incident-to billing rules. Medicare incident-to billing allows an APP to render a service "incident to" a physician's plan of care and bill at 100% of the physician fee schedule (vs 85% direct APP billing) when the strict conditions are met: physician initiated the plan of care, physician is on-premises and immediately available, the APP is following the established plan, and the visit is a follow-up not a new problem. This must be documented or the claim is at risk under audit. Many APPs do not bill incident-to even when eligible because the documentation burden is non-trivial — an AI scribe that captures the incident-to elements supports compliant documentation when CMS conditions are met.
- Split/shared visit documentation (CMS 2024+). In hospital settings (E&M codes 99221-99239 inpatient, 99281-99285 ED), CMS 2024 rules require the substantive portion (medically necessary history, exam, MDM, or more than half of total time) to be performed by the practitioner of record (physician or APP) with documentation showing who performed what. The AI must support this attribution to comply with payment rules and prevent denied claims.
- Care management and transitional care codes. CCM (99490 chronic care management 20+ minutes/month, 99487 complex CCM 60+ minutes/month, 99491 physician/APP-delivered CCM, G0506 add-on for comprehensive assessment), TCM (99495 moderate complexity within 14 days, 99496 high complexity within 7 days), Principal Care Management (99424-99427), Behavioral Health Integration (99484, 99492-99494). These codes require structured time-based documentation of qualifying activities and are typically billed by APPs or physicians but performed largely by RN care managers, MAs, and BH consultants. The note must capture activity, time, and clinical decision-making contribution.
- Interdisciplinary care plans. PCMH-recognized practices and ACOs document interdisciplinary care plans that include problem list, goals, interventions, and team roles across MD/APP, RN, MA, BH, RD, social work. The plan is a living document that evolves with team input. A single-encounter scribe captures the visit but not the team-coordinated longitudinal care plan.
- Social Determinants of Health documentation. SDoH screening (PRAPARE, AHC HRSN, Z-codes Z55-Z65) is now required in many quality programs and is increasingly documented by MAs or RNs at intake, with social work intervention. Z-codes for housing instability, food insecurity, transportation, and interpersonal violence have measurable revenue and quality-program impact under HCC risk adjustment in MA/ACO contexts.
Audit, Quality, and Reimbursement Stakes
Audit risk is distributed across the team. Incident-to claims are scrutinized by Medicare audits and OIG reviews, with documentation deficiencies producing recoupments. Split/shared visits in hospital settings are a high-volume CMS audit target since the 2024 rule update. Care management codes (CCM, TCM, PCM) have specific time-based documentation requirements that audit reviewers verify by matching log entries to the chart. PCMH and ACO programs link documentation completeness to shared-savings distributions. SDoH Z-codes increasingly affect HCC RAF scores and per-member-per-month payment in MA and ACO contexts.
A team-wide AI scribe that tags rendering provider role, captures incident-to elements, supports split/shared substantive-portion documentation, structures care management activities, and supports SDoH screening directly affects revenue capture, audit defensibility, and quality-program performance.
Quick Comparison — Top AI Scribes for Medical Professionals
| Rank | Tool | Price | Multi-Role Support | EHR Integration | Best For |
|---|---|---|---|---|---|
| 1 | DeepCura | $129/mo | Custom role/scope templates + CDS | Epic, Cerner, athenahealth, AdvancedMD, eClinicalWorks (9 EHRs) | Best Overall |
| 2 | Freed AI | $39-$104/mo | NP/PA-friendly | Browser-based; limited APP-specific structure | Solo APPs |
| 3 | Abridge AI | Custom enterprise | Health-system multi-role | Epic deep integration | Large health systems |
| 4 | Nuance DAX Copilot | Custom enterprise | Multi-role, EHR-driven | Epic, Cerner deep | Epic/Cerner shops |
| 5 | DeepScribe | ~$99-$149/mo | Customizable templates | Limited multi-role | Mid-size practices |
| 6 | Heidi Health | $0-$99/mo | Multi-role templates | Limited write-back | Free credentialing trial |
For a broader cross-specialty comparison, see our Best AI Medical Scribes in 2026 ranking. For physician-specific tool selection, see our best AI scribe for physicians guide.
What to Look For in an AI Scribe for Medical Professionals
CMS billing rules summarized below are general background only. Verify against current CMS Medicare Learning Network articles, the CPT® manual, and your compliance officer before billing decisions. DeepCura's tool documents observed encounters; it does not enable billing for services not actually rendered under required supervision conditions.
Care-team documentation is fundamentally multi-role. Before choosing a tool, evaluate it against these eight criteria:
1. Rendering Provider and Role Tagging. The AI must tag every note with the credentialing role (MD, DO, NP, PA, RN, CNM, CRNA, MA, RD, MSW, RPh) and the supervising/collaborating physician where applicable. This drives downstream billing rules, scope documentation, and audit defensibility. A scribe that produces notes attributed only as "provider" without role specificity creates compliance risk.
2. Incident-to Documentation Support. The AI should capture the incident-to elements: physician's initial plan of care reference, physician on-premises and immediately available statement, APP following the established plan, follow-up not new-problem encounter type. Templates should make incident-to documentation fast and complete so the encounter is documented accurately. Medicare's incident-to billing requirements (physician initiated plan of care, on-premises supervision, established plan, follow-up) must all be met independently of the documentation tool.
3. Split/Shared Visit Substantive Portion. For hospital E&M (99221-99239 inpatient, 99281-99285 ED), the AI should support documenting which provider (physician or APP) performed the substantive portion of the visit per CMS 2024 rules — either the medically necessary history, exam, MDM, or more than half of total time. Documentation must explicitly attribute the substantive portion to the billing provider.
4. Care Management Code Capture (CCM, TCM, BHI, PCM). Structured time-based documentation of qualifying activities for 99490 (CCM 20-39 min), 99491 (CCM 30-39 min physician/APP), 99437 (CCM each additional 30 min), 99487 (Complex CCM 60+ min), 99489 (Complex CCM each add'l 30 min), G0506, 99495 (TCM moderate), 99496 (TCM high), 99424-99427 (PCM), 99484 (BHI), 99492-99494 (Collaborative Care Model). Time, qualifying activity, and clinical decision-making contribution must be captured.
5. Interdisciplinary Team Care Plan Templates. Templates that support team-based care plan documentation — problem list with team-assigned interventions, BH consultant input, RN care management input, RD nutrition counseling input, MSW SDoH and resource navigation input — coalesced into a longitudinal plan visible across team members.
6. SDoH Screening and Z-Code Documentation. Templates for PRAPARE or AHC HRSN screening with Z55-Z65 Z-code generation (Z59.0 housing instability, Z59.4 food insecurity, Z60.2 social isolation, Z62.21 ACE childhood maltreatment history, Z63.0 problems in primary support group, Z65.4 victim of crime or terrorism). Integration into HCC risk adjustment workflows.
7. PCMH and ACO Quality Measure Support. Templates structured to capture PCMH 2024 standards (continuous QI, patient-centered access, team-based care, knowing and managing patients, care management and support, care coordination and transitions, performance measurement) and ACO quality measures (ACO 1 risk-standardized hospital admissions, ACO 11 falls, ACO 14 BMI screening, ACO 17 depression remission, ACO 18 diabetes A1C control).
8. Multi-EHR Integration. Bidirectional integration with Epic, Cerner (Oracle), athenahealth, eClinicalWorks, AdvancedMD, NextGen, Allscripts, Greenway, MEDITECH, and Practice Fusion — the EHRs that span primary care, FQHC, hospital outpatient clinic, urgent care, and specialty practice settings where multi-role teams operate.
Detailed Reviews
1. DeepCura — Best Overall for the Clinical Care Team
DeepCura is a customizable clinical AI platform combining ambient scribing, clinical decision support, evidence search, practice automation, and bidirectional EHR integration — $129/month with unlimited notes. For multi-role clinical care teams — primary care practices with physicians, NPs, PAs, MAs, and RNs; FQHCs with integrated BH and care management; PCMH-recognized practices; ACO participants; rural health clinics — DeepCura's combination of customizable templates, role-aware structure, and unlimited per-user notes delivers strong value across the full team.
For multi-role teams, the key differentiators are template flexibility and credit-based access tiering. DeepCura's custom template builder lets practice managers encode role-specific templates: a physician E&M visit with full MDM structure for 99202-99215; an NP independent visit with the same E&M structure plus full-practice-authority scope tagging or collaborative-agreement supervision documentation; a PA visit with collaborative-agreement and supervising-physician tagging; an MA intake summary with vitals, ROS by chief complaint, screening tools (PHQ-9, GAD-7, AUDIT, ACE, PRAPARE), and prep for the rendering provider; an RN care management call template with TCM and CCM time tracking; an RD nutrition counseling note with MNT (medical nutrition therapy) goals; an MSW SDoH and care coordination template with Z-code generation. All templates feed into a coherent shared chart with clear rendering-provider attribution.
CDS Mode (3 credits per note) generates differential considerations alongside the note — particularly valuable for APPs in primary care who carry broad-differential presentations (chest pain, abdominal pain, fatigue, headache, dizziness) where the documented differential supports both clinical reasoning and medicolegal defense.
DeepEvidentia — DeepCura's evidence search engine — pulls from PubMed, USPSTF recommendations, FDA drug labels, CMS billing guides, AHRQ practice guides, and NCQA PCMH standards. Useful for APPs working in unfamiliar specialty contexts, RN care managers preparing population health outreach, and care coordinators looking up resource pathways.
Strengths:
- Custom templates per role (MD/DO, NP, PA, MA, RN, RD, MSW, RT, PharmD) with role tagging in every note
- Incident-to documentation support with structured fields for physician plan of care, supervision, and APP follow-up
- Split/shared visit documentation for hospital E&M with substantive-portion attribution
- Care management templates for CCM (99490/99487/99491), TCM (99495/99496), PCM (99424-99427), BHI (99484), Collaborative Care (99492-99494)
- SDoH screening templates with Z-code generation and HCC risk-adjustment workflow integration
- AI receptionist for after-hours triage and intake routing — particularly valuable for primary care teams with limited evening front-desk coverage
- CDS Mode with differentials for APP broad-differential encounters (3 credits per note)
- DeepEvidentia evidence search across clinical, regulatory, and operational queries
- Multiple AI engines matched to encounter complexity (1-15 credits)
- Unlimited notes per provider on all plans
- Bidirectional integration with Epic, Cerner, athenahealth, AdvancedMD, eClinicalWorks, NextGen, Allscripts, Greenway, Practice Fusion
Limitations:
- Custom template builder requires meaningful initial setup time (8-15 hours for a multi-role primary care practice to encode templates per role)
- Scope-of-practice and incident-to compliance is the practitioner's responsibility — the AI structures the documentation but does not legally substitute for credentialing or scope verification
- CDS Mode trained on broad medical literature — specialty- or role-specific differentials require validation by the practitioner
Pricing: $129/month per provider — all features included. Free trial available, no credit card required.
Verdict: DeepCura is a strong choice for multi-role clinical care teams that want one platform handling physician notes, APP notes (NP/PA), MA intake, RN care management, RD nutrition counseling, and MSW SDoH documentation. The flexibility cost is upfront setup time, but for PCMH-recognized practices, ACO participants, FQHCs, and primary care practices managing CCM and TCM revenue streams, the per-role template depth delivers value that single-role scribes cannot match.
DeepCura: AI Scribe for the Full Clinical Care Team
Role-specific templates for MD, NP, PA, MA, RN, RD, MSW; incident-to and split/shared documentation; CCM/TCM/PCM/BHI templates; SDoH screening with Z-code generation — $129/mo, unlimited notes per user. Start your free trial.
+1 (415) 549-1829Available 24/7 · Set up in seconds · No credit card required
2. Freed AI — Best for Solo NPs and PAs
Freed AI is a clean, fast ambient scribe with a tiered Free-to-Premier pricing structure popular among solo and early-career NPs and PAs in primary care, urgent care, and outpatient specialty settings. The price point ($39-$104/month), short learning curve, and focus on rapid SOAP-note generation make it well-suited to APPs working in fee-for-service environments where speed-to-note is the primary value driver.
For solo APPs, Freed handles the basic encounter capture and SOAP note structure cleanly. The Premier tier ($104/month) adds EHR push and ICD-10 coding suggestions, which addresses the highest-volume APP workflow friction. APPs in collaborative-agreement states report that Freed's note quality is sufficient for routine encounters and the time savings are meaningful.
The limitation for multi-role teams is that Freed is single-provider focused. There is no incident-to template, no split/shared substantive-portion documentation, no CCM/TCM time-tracking, no SDoH Z-code generation, and no PCMH/ACO quality measure structure. For solo APPs whose practice does not engage these workflows, Freed is more than adequate. For APPs in PCMH-recognized practices, ACOs, or FQHCs where team-based care documentation is required, Freed leaves significant documentation gaps that other team members must fill manually.
Pricing: $39/month (Starter, 40 notes), $79/month (Core, unlimited), $104/month (Premier, unlimited + EHR push + ICD-10).
Verdict: Best for solo NPs, PAs, and CNMs in fee-for-service primary care, urgent care, or outpatient specialty practice who want a fast ambient scribe at an accessible price. Not the right fit for multi-role teams in PCMH, ACO, or FQHC contexts. Read our Freed AI review.
3. Abridge AI — Best for Large Health Systems
Abridge has emerged as the leading enterprise AI scribe for large health systems, with deployments at multiple major academic medical centers and integrated delivery networks. The product is sold via custom enterprise contracts and includes deep integration with Epic — covering inpatient, outpatient, and emergency department workflows for the full care team (attendings, residents, fellows, APPs, RNs in care management roles).
For health systems with thousands of providers across multiple specialties and roles, Abridge offers consistent scribing infrastructure with role-aware templates, IDS/EDC integration, hospital-specific workflows (admit notes, transfer notes, discharge summaries), and the IT/security/legal frameworks that enterprise procurement requires. The product is well-tuned for the operational scale and compliance constraints of academic medical centers and large community health systems.
The limitation is access — Abridge is not sold to small or mid-size independent practices. Pricing is custom enterprise (typically per-provider per-month with multi-year contracts and custom implementation fees), and the product is positioned for organizations with dedicated IT, training, and change-management resources. For a 2-15 provider independent practice, Abridge is not in the consideration set.
Pricing: Custom enterprise contracts. Not publicly disclosed. Multi-year minimum.
Verdict: Best for large health systems and IDS/EDC organizations with Epic deep integration requirements, multi-role/multi-setting deployment, and enterprise procurement processes. Not available to small independent practices. Read our Abridge AI review.
4. Nuance DAX Copilot — Best for Deep Epic / Cerner Integration
Nuance DAX Copilot (acquired by Microsoft in 2022) is the incumbent enterprise AI scribe with extensive Epic and Cerner integration in the market — a function of Nuance's history as the dominant medical voice recognition vendor and the Microsoft ecosystem leverage post-acquisition. DAX Copilot supports multi-role teams in health-system contexts and integrates ambient documentation directly into the Epic Hyperdrive and Cerner workflows.
For health systems already on Microsoft enterprise contracts (M365, Azure, Teams), DAX Copilot is the path-of-least-procurement-resistance and offers consistent infrastructure across the organization. The product handles physician, APP, and care management role documentation with EHR-native integration that lower-tier scribes cannot match.
The limitations parallel Abridge: enterprise-only pricing, multi-year contracts, custom implementation, and IT/training overhead. Not accessible to small independent practices.
Pricing: Custom enterprise. Multi-year contracts.
Verdict: Best for health systems on Microsoft enterprise contracts with Epic or Cerner who want deep EHR-native integration. See our DeepCura vs Nuance DAX Copilot comparison for a detailed look.
5. DeepScribe — Best Customizable for Mid-Size Practices
DeepScribe offers ambient AI documentation with a customizable template engine that mid-size practices use for multi-role workflows. Practice managers build templates for MD, NP, PA, and RN roles with appropriate field structures, and the AI populates them from ambient capture. DeepScribe sits between the high-end enterprise tools (Abridge, Nuance) and the low-end solo tools (Freed, Heidi) in capability and price.
For mid-size primary care practices and specialty groups (15-50 providers) running mixed MD/APP teams, DeepScribe's customization flexibility supports role-aware templates and basic care-management workflows. EHR integration depth varies by EHR — Epic and Cerner integrations are improving but not at the depth of Abridge or Nuance.
Pricing: Approximately $99-$149/month range. Custom enterprise pricing for larger practices.
Verdict: Solid mid-tier option for mid-size practices comfortable with template engineering effort. Less out-of-box than Freed for solo APPs, less enterprise-grade than Abridge or Nuance for health systems, but a credible middle path. Read our DeepScribe review.
6. Heidi Health — Best Free Tier for Credentialing Trial
Heidi Health offers a usable free tier (limited notes per month) that lets individual providers and small teams test ambient AI documentation at zero cost before paid plans kick in at the Pro level. Heidi has multi-role templates available across specialties and works for both MDs and APPs. International product traction in Australia, NZ, and the UK is stronger than US, but the templates support standard SOAP/E&M documentation that crosses borders.
EHR integration is limited (clipboard or email), but for trial-phase evaluation across team roles, the free tier is the most accessible entry point. US teams running full caseloads typically outgrow the free tier within the first month.
Pricing: Free tier (limited notes), Pro tier roughly $129/month, enterprise tier higher.
Verdict: Best for solo providers or small teams who want to test ambient AI documentation at zero cost across multiple roles before committing to a paid tool. Read our Heidi Health review.
Head-to-Head — Medical Team Documentation Features
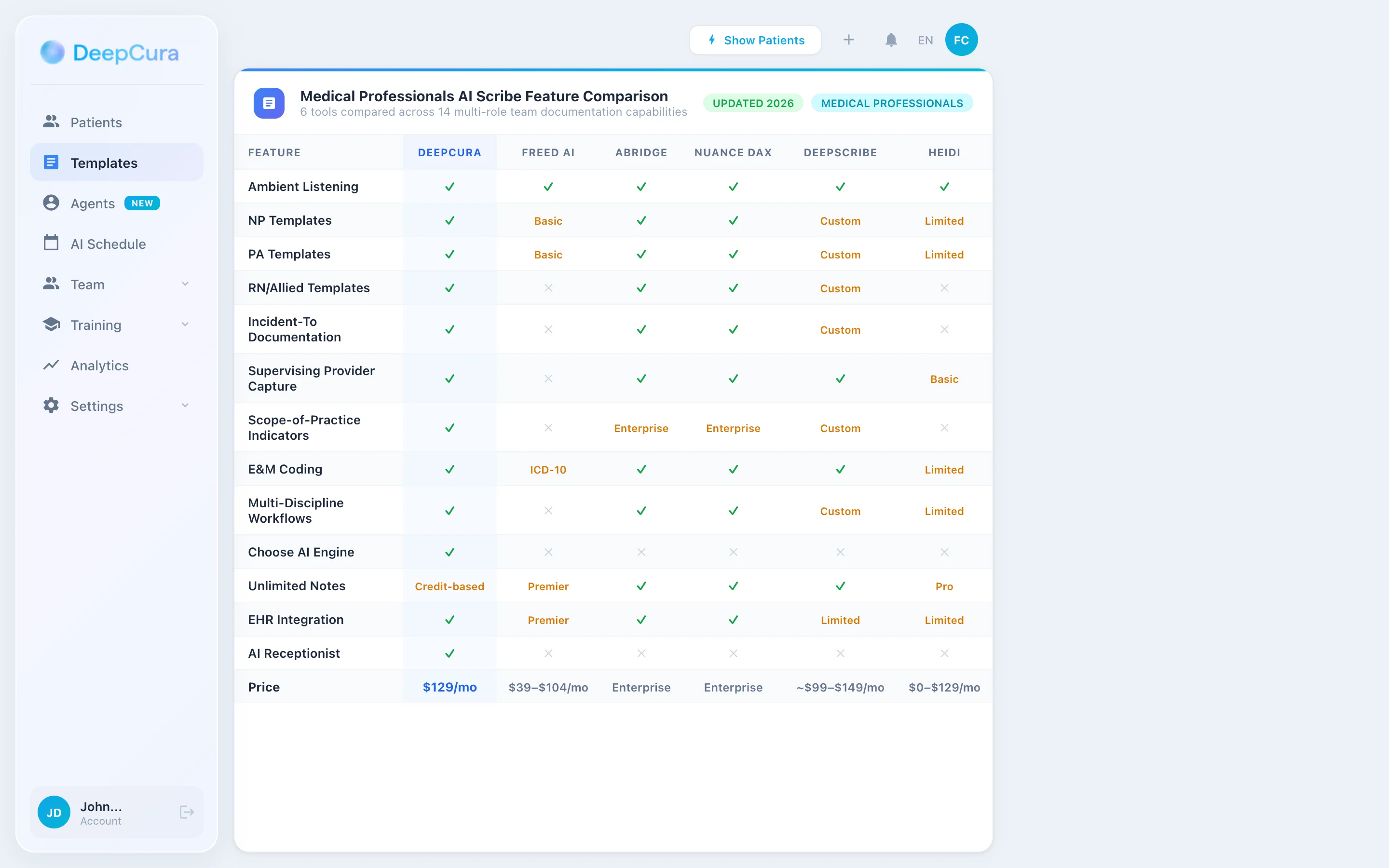
| Feature | DeepCura | Freed | Abridge | Nuance DAX | DeepScribe | Heidi |
|---|---|---|---|---|---|---|
| Multi-Role Templates (MD/NP/PA/MA/RN/RD/MSW) | ✓ Custom | NP/PA basic | ✓ Enterprise | ✓ Enterprise | Custom | Limited |
| Rendering Provider Tagging | ✓ | Basic | ✓ | ✓ | ✓ | Basic |
| Incident-to Documentation | ✓ structured | ✗ | ✓ Enterprise | ✓ Enterprise | Custom | ✗ |
| Split/Shared Visit (CMS 2024) | ✓ | ✗ | ✓ | ✓ | Custom | ✗ |
| CCM / TCM / PCM / BHI Templates | ✓ | ✗ | ✓ Enterprise | ✓ Enterprise | Custom | ✗ |
| Collaborative Care (99492-99494) | ✓ | ✗ | ✓ | ✓ | Custom | ✗ |
| SDoH Screening + Z-Codes | ✓ | ✗ | ✓ | ✓ | Custom | ✗ |
| HCC RAF Capture | ✓ | ICD-10 only | ✓ | ✓ | Custom | Limited |
| PCMH / ACO Quality Templates | ✓ | ✗ | ✓ | ✓ | Custom | ✗ |
| AI Receptionist (after-hours) | ✓ | ✗ | ✗ | ✗ | ✗ | ✗ |
| Clinical Decision Support | ✓ (differentials) | ✗ | Limited | ✗ | ✗ | ✗ |
| Evidence Search | ✓ (DeepEvidentia) | ✗ | ✗ | ✗ | ✗ | ✗ |
| EHR Bidirectional | 9 EHRs | Browser scrape (Premier) | Epic deep | Epic/Cerner deep | Limited | Limited |
| Price | $129/mo all features | $39-$104/mo | Enterprise custom | Enterprise custom | $99-$149/mo | $0-$99/mo |
Interdisciplinary Team Workflow with DeepCura
DeepCura's tiered credit system lets care teams match AI resources to documentation complexity — fast for routine encounters, deeper for care management and complex IDT documentation.
Routine APP/Physician Visit (1 Credit) — 99213/99214/99215 Established Patient
For routine 15-minute established-patient visits in primary care — well-controlled HTN, T2DM follow-up, anxiety follow-up, URI, low-back pain, contraception management — the 1-credit model generates a complete E&M-coded note in under 30 seconds with HPI, ROS, exam, MDM, and plan. Speed-optimized for the 18-22 patient day where APPs and physicians need note completion to keep up with throughput.
Complex IDT Visit (3 Credits CDS) — 99214/99215 with Care Management Touch
For visits that include care management activities — multi-condition management, social work consultation referral, RD nutrition counseling order, BH integrated consultation, transitions of care — CDS Mode generates differential considerations and structures the IDT plan with team role attributions. CCM/TCM/BHI time tracking initiates from the visit and propagates to the appropriate team member's care management documentation.
Hospital Split/Shared and Care Management (15 Credits) — 99221-99239 Inpatient, Complex CCM
For inpatient admit notes, transfer notes, discharge summaries, and complex care management cases — multi-attendings, residents, APPs in a teaching hospital; substantive-portion attribution under CMS 2024; CCM 99487 with 60+ minutes/month across team members — the maximum-depth model produces complete narratives with attribution, time tracking, and IDT plan integration. The complexity of multi-provider attribution and time aggregation justifies the deeper compute.
One Platform for the Full Care Team
Templates for MD, NP, PA, MA, RN, RD, MSW with rendering-provider tagging, incident-to support, split/shared substantive-portion attribution, and CCM/TCM/PCM/BHI capture — DeepCura keeps the team's chart coherent. Start your free trial.
+1 (415) 549-1829Available 24/7 · Set up in seconds · No credit card required
Clinical Decision Support and Evidence Search for the Care Team
CDS Mode outputs are documentation-aid suggestions for clinician review. They are not diagnoses, treatment recommendations, or substitutes for clinical judgment. The clinician retains full responsibility for diagnosis, workup, and treatment decisions. DeepCura is not an FDA-cleared medical device.
CDS Mode — Differentials Across Roles
APPs in primary care carry the same broad-differential encounters as physicians and benefit equally from documented differential generation. RN care managers handling phone triage encounter symptom-driven calls (chest pain, shortness of breath, headache, abdominal pain) where structured triage decision support reduces both miss rate and unnecessary ED referrals. CDS Mode supports both clinician roles with differential generation calibrated to the encounter type.
For an NP managing a 65-year-old with poorly controlled T2DM, hypertension, and new-onset peripheral neuropathy, CDS Mode flags: diabetic peripheral neuropathy (most likely given duration and HbA1c), B12 deficiency from metformin (rule-out indication), CKD-related neuropathy (correlates with eGFR), and lumbosacral radiculopathy (positional and dermatomal pattern). The differential informs the workup (B12, eGFR, A1C, monofilament exam) and supports the documented clinical reasoning that audits and quality programs require.
DeepEvidentia — Evidence at the Bedside for Any Role
DeepEvidentia provides real-time access to PubMed, USPSTF recommendations, FDA drug labels, CMS billing guides, AHRQ practice guides, NCQA PCMH standards, ACO quality measures, and HEDIS specifications.
Example queries clinical care team members actually ask:
- "Incident-to billing requirements for new vs established patients" — returns CMS Manual System Pub. 100-04 Chapter 12 §60.1 with current rules
- "CCM 99490 vs 99491 distinction by who provides the service" — returns CMS Care Management Services Booklet (ICN 909188) with billing rules
- "USPSTF colorectal cancer screening recommendation for 45-49 year olds" — returns the Grade B 2021 update
- "Z-codes for SDoH housing instability and food insecurity in HCC RAF" — returns Z59.0, Z59.4 with HCC mapping notes
- "ACO quality measures 2026 — depression remission specifications" — returns ACO 17 specifications and exclusion logic
- "Beers Criteria for benzodiazepine prescribing in 65+ patients" — returns AGS 2023 update with avoid recommendations
For a multi-role care team, the value is breadth — the same evidence engine answers a clinical question from an NP, a billing/scope question from a practice administrator, a quality-measure question from a care manager, and a regulatory question from a compliance officer.
Pricing Comparison
| Tool | Monthly | Note Limit | Multi-Role | Best Plan |
|---|---|---|---|---|
| DeepCura | $129/mo | Unlimited | ✓ Custom roles | Single plan, all features |
| Freed AI | $39-$104/mo | 40-unlimited | NP/PA basic | Premier ($104) |
| Abridge AI | Enterprise custom | Enterprise | ✓ | Enterprise contract |
| Nuance DAX Copilot | Enterprise custom | Enterprise | ✓ | Enterprise contract |
| DeepScribe | ~$99-$149/mo | Unlimited | Custom | Standard plan |
| Heidi Health | $0-$99/mo | Free tier limited | Limited | Free or Pro |
See DeepCura in Action
Watch how DeepCura handles the full clinical team workflow — physician notes, NP/PA notes with incident-to and split/shared documentation, MA intake, RN care management with CCM/TCM time tracking, MSW SDoH and Z-code documentation, evidence search via DeepEvidentia, and AI receptionist for after-hours triage.

Frequently Asked Questions
What is the best AI scribe for medical professionals?
DeepCura is a strong cross-functional choice for multi-role clinical care teams that want one platform handling physicians, NPs, PAs, MAs, RNs, RDs, and MSWs with role-specific templates, rendering-provider tagging, incident-to documentation, split/shared visit support, and CCM/TCM/PCM/BHI capture. For solo NPs and PAs in fee-for-service practice without team-based care requirements, Freed AI is the leading accessible-price option. For large health systems with Epic deep integration requirements, Abridge AI and Nuance DAX Copilot are the enterprise leaders.
Do AI scribes support incident-to billing documentation for NPs and PAs?
DeepCura supports structured incident-to documentation with fields for the physician's initial plan of care, physician on-premises and immediately available statement, APP follow-up not new-problem encounter type, and supervising-physician tagging. Enterprise tools (Abridge, Nuance DAX Copilot) support incident-to in their respective workflows. Solo-focused tools (Freed, Heidi) do not have native incident-to template support — practices using these tools manually add the incident-to language. Compliance with incident-to rules is the practitioner's and practice's responsibility; the AI structures the documentation but does not legally substitute for scope verification.
Do AI scribes support split/shared visit documentation under CMS 2024 rules?
DeepCura, Abridge, and Nuance DAX Copilot support split/shared visit documentation with substantive-portion attribution per CMS 2024 rules — either the medically necessary history, exam, MDM, or more than half of total time documented for the billing provider. Solo-focused tools do not have native split/shared support. Hospital systems using mixed physician/APP coverage in inpatient and ED settings should select tools that support this attribution to maintain claim defensibility.
Can AI scribes capture CCM, TCM, PCM, and BHI time-based documentation?
DeepCura supports CCM (99490, 99437, 99491, 99487, 99489), TCM (99495, 99496), PCM (99424-99427), BHI (99484), and Collaborative Care Model (99492-99494) with structured time tracking, qualifying activity capture, and team-role attribution. Enterprise tools (Abridge, Nuance DAX Copilot) support these in their respective workflows. Solo-focused tools (Freed, Heidi) do not have native care management code support.
Do AI scribes integrate with Epic, Cerner, athenahealth, and AdvancedMD?
DeepCura integrates with Epic, Cerner, athenahealth, AdvancedMD, eClinicalWorks, NextGen, Allscripts, Greenway, and Practice Fusion via bidirectional API integration. Abridge and Nuance DAX Copilot have extensive Epic and Cerner integration in the enterprise market. Freed offers EHR push at the Premier tier ($104/month). DeepScribe has improving but variable integration depth. Heidi pushes via clipboard or email.
Can AI scribes document SDoH screening and Z-codes for HCC risk adjustment?
DeepCura supports SDoH screening templates (PRAPARE, AHC HRSN) with Z55-Z65 Z-code generation (Z59.0 housing instability, Z59.4 food insecurity, Z60.2 social isolation, Z62.21 ACE childhood maltreatment, Z63.0 problems in primary support, Z65.4 victim of crime) and integration into HCC risk adjustment workflows. Enterprise tools support SDoH at the platform level. Solo-focused tools do not have native SDoH screening templates — practices typically use external SDoH tools and manually code Z-codes into the chart.
How much do AI scribes for medical professionals cost?
Pricing ranges from a free Heidi tier through enterprise. Freed AI runs $39-$104/month per user. Heidi Pro is approximately $99/month. DeepScribe is $99-$149/month. DeepCura is $129/month per provider with unlimited notes, CDS, evidence search, AI receptionist, multi-role templates, and full feature access. Enterprise tools (Abridge, Nuance DAX Copilot) are custom-priced with multi-year contracts. For most independent multi-role practices and FQHCs in the 5-50 provider range, the $99-$150/month accessible-price tier delivers the best feature-to-cost ratio.
Are AI scribes HIPAA-compliant for use across the full clinical care team?
Reputable AI scribes operate under HIPAA Business Associate Agreements with encryption in transit and at rest. Multi-role team deployment requires that the BAA cover all credentialed roles with appropriate access controls (RN-level access, MA-level access, BH-level access with 42 CFR Part 2 considerations). DeepCura, Abridge, Nuance DAX Copilot, and DeepScribe provide BAAs with role-based access controls. Freed and Heidi provide BAAs at appropriate plan tiers — verify role-based access requirements during procurement.
Final Verdict
For multi-role clinical care teams, the choice comes down to four profiles:
Best overall: DeepCura at $129/month — customizable role-specific templates (MD, NP, PA, MA, RN, RD, MSW), incident-to and split/shared documentation, CCM/TCM/PCM/BHI capture, SDoH screening with Z-codes, AI receptionist for after-hours triage, CDS differentials, evidence search, and unlimited notes per provider. A strong choice for PCMH-recognized practices, ACO participants, FQHCs, and primary care practices managing care management revenue streams.
Best for solo APPs: Freed AI at $39-$104/month — accessible-price ambient scribe well-suited to solo NPs, PAs, and CNMs in fee-for-service practice without team-based care requirements.
Best for large health systems: Abridge AI and Nuance DAX Copilot — enterprise-grade with deep Epic and Cerner integration, multi-role/multi-setting deployment, and the IT/security/legal frameworks that academic medical centers and large IDS/EDC organizations require. Custom enterprise pricing with multi-year contracts.
Best for free-tier credentialing trial: Heidi Health — free tier (limited notes) lets teams test ambient AI documentation across roles before paid plans kick in.
For a broader cross-specialty comparison, see our Best AI Medical Scribes in 2026 ranking. For physician-specific tool selection, see our best AI scribe for physicians guide. For practices that need after-hours phone automation, see our Best AI Medical Receptionist guide. For clinical AI chat tools, see Best ChatGPT for Doctors. For free copy-paste clinical templates, see our SOAP note template guide. If you are evaluating EMRs alongside the scribe decision, see our best EMR for small practices ranking. For specialty-specific deep dives, see best AI scribe for emergency medicine, best AI scribe for psychiatry, and best AI scribe for veterinarians.
References
[1] Sinsky CA, Colligan L, Li L, Prgomet M, Reynolds S, Goeders L, Westbrook J, Tutty M, Blike G, "Allocation of physician time in ambulatory practice: A time and motion study in 4 specialties," Annals of Internal Medicine, 165(11), 753-760, 2016. pubmed.ncbi.nlm.nih.gov/27595430
[2] Arndt BG, Beasley JW, Watkinson MD, Temte JL, Tuan WJ, Sinsky CA, Gilchrist VJ, "Tethered to the EHR: Primary care physician workload assessment using EHR event log data and time-motion observations," Annals of Family Medicine, 15(5), 419-426, 2017. pubmed.ncbi.nlm.nih.gov/28893811
[3] National Academy of Medicine, "Action Collaborative on Clinician Well-Being and Resilience," NAM. nam.edu/initiatives/clinician-resilience-and-well-being
[4] Centers for Medicare & Medicaid Services, "Medicare Claims Processing Manual, Chapter 12 — Physicians/Nonphysician Practitioners," CMS Pub. 100-04. cms.gov/regulations-and-guidance/guidance/manuals
[5] Centers for Medicare & Medicaid Services, "Care Management Services in Rural Health Clinics and Federally Qualified Health Centers — CCM, TCM, PCM, BHI, Psychiatric Collaborative Care," CMS MLN. cms.gov/outreach-and-education/medicare-learning-network-mln
[6] Centers for Medicare & Medicaid Services, "Calendar Year (CY) 2024 Medicare Physician Fee Schedule Final Rule — Split (or Shared) Visits," CMS-1784-F, 2023. cms.gov/medicare/payment/fee-schedules/physician
[7] American Association of Nurse Practitioners, "State Practice Environment — NP Scope of Practice," AANP. aanp.org/advocacy/state/state-practice-environment
[8] American Academy of PAs, "Optimal Team Practice and PA Scope of Practice," AAPA. aapa.org/advocacy-central/optimal-team-practice
[9] National Committee for Quality Assurance, "Patient-Centered Medical Home (PCMH) 2024 Standards," NCQA. ncqa.org/programs/health-care-providers-practices/patient-centered-medical-home-pcmh
[10] Centers for Medicare & Medicaid Services, "Medicare Shared Savings Program — Quality Measures and Performance Standards," CMS. cms.gov/medicare/medicare-fee-for-service-payment/sharedsavingsprogram
[11] Agency for Healthcare Research and Quality, "Social Determinants of Health Database and PRAPARE Documentation," AHRQ. ahrq.gov/sdoh