Urgent care providers commonly see a high volume of patients per shift across one of the broadest acute presentation mixes in medicine — viral URI and pharyngitis with strep RADT or RSV/flu/COVID screening, acute injuries requiring laceration repair (12001-13160), splinting (29105-29515) and casting (29065-29086), foreign body removal (10120/10121 for skin/subcutaneous; eye, ear-canal, and nasal FB use separate code families such as 65205-65222, 69200/69205, and 30300), abscess I&D (10060/10061/10080/10081), simple and complex wound care, joint injections for acute injury, work injury triage with first-report-of-injury documentation, DOT physicals (CMV driver medical examinations using FMCSA Form MCSA-5875), school and sports physicals, pre-employment physicals, and a differential breadth that resembles a compressed ED encounter. Documentation must support both the medical record and the work-comp claim, the DOT certification, the school sports clearance, the pre-op clearance, or the discharge to follow-up — and throughput pressure is high. Vendor-reported documentation times reflect testing conditions and vary materially by visit type, EHR, and clinician workflow.
We ranked 6 AI scribes on the criteria that matter most for urgent care documentation:
- Acute presentation differential and disposition documentation — does the AI support the broad-and-fast differential generation that urgent care requires (chest pain workup with cardiac vs MSK vs pulmonary differential, abdominal pain with surgical vs medical differential and red flag screening, headache with primary vs secondary differential), and structure disposition (treat and release, transfer to ED, admit, follow-up)?
- Procedural CPT capture — does it document simple laceration repair by region and length (12001-12007 trunk/extremities; 12011-12018 face/ear/eyelid/nose/lip/mucous membrane), intermediate repair requiring layered closure (12031-12057), and complex repair (13100-13160); splinting (29125 short arm, 29130 finger, 29515 short leg), casting (29065 shoulder-to-hand, 29075 elbow-to-finger, 29085 hand-and-lower-forearm, 29086 finger-cast), abscess I&D (10060 simple, 10061 complex, 10080/10081 pilonidal cyst), skin/subcutaneous foreign body removal (10120 simple, 10121 complex; eye/ear/nasal FB use separate code families — e.g., 65205-65222, 69200/69205, 30300), nail trephination (11740), and nail avulsion (11730/11732)?
- Work-comp DWC and occupational medicine documentation — does it produce work-comp first-report-of-injury narratives with mechanism of injury detail, work status determination (full duty, modified duty with specific restrictions, off-work), DWC forms (state-specific — California DWC-1 / DWC-PR-2; Texas DWC-69 / DWC-73; Florida DFS-F5-DWC-25), and DOT/FAA/USCG occupational physical documentation?
- DOT exam, sports physical, and pre-employment exam templates — does it support FMCSA Form MCSA-5875 CMV driver medical examination, AAP/AHA pre-participation sports examination form, school physical templates, and pre-employment physical examination structures?
All products were evaluated in February-April 2026. Pricing reflects publicly available rates. Urgent care is a high-throughput, broad-presentation setting where ambient capture quality and procedural documentation depth matter more than longitudinal chronic disease management depth.
Disclosure & methodology. This comparison is published by DeepCura, which is included in the ranking. Pricing and feature claims for competitor products reflect publicly available information as of the evaluation period above and may change — verify directly with each vendor before procurement. This article is editorial commentary; it is not medical, legal, billing, or compliance advice. CPT® is a registered trademark of the American Medical Association. UCA, NUCC, EMTALA, OSHA, DOT, and other organization names referenced are trademarks or marks of their respective owners; DeepCura is not affiliated with or endorsed by these organizations. References are nominative and used for descriptive comparison only.
Why Urgent Care Needs an AI Scribe
The Documentation Reality in an Urgent Care
Urgent care occupies a unique position in the documentation landscape — broader than primary care in differential diagnosis (every body system, every age group, every acuity short of true emergency), narrower than emergency medicine in disposition options, with significant procedural volume that primary care typically does not see, and with a regulatory documentation burden (work-comp, DOT, sports physicals, school physicals) that primary care typically does not handle at urgent-care volume.
A typical urgent care provider on a 12-hour shift documents:
- 20-40 acute medical visits — viral URI/pharyngitis (J06.9, J02.9, J20.9), influenza (J11.x), COVID (U07.1), strep pharyngitis (J02.0) with RADT result, otitis media (H66.9), sinusitis (J01.x, J32.x), conjunctivitis (H10.x), urinary tract infection (N39.0) with UA result, acute gastroenteritis (K52.x), simple skin/soft tissue infection (L03.x cellulitis), abscess (L02.x), allergic reaction (T78.x), asthma exacerbation (J45.x), COPD exacerbation (J44.x), uncomplicated chest pain in low-risk patient (R07.x with workup justification), uncomplicated abdominal pain (R10.x with red flag screening), headache (R51, G44.x with secondary headache rule-out), back pain (M54.x with red flag screening), and the long tail of presentations that don't fit a clean primary care follow-up but don't justify ED transfer
- 5-15 procedural visits — laceration repair, abscess I&D, foreign body removal, simple fracture splinting before orthopedic referral, nailbed injury management, eye irrigation and FB removal, ear canal lavage and FB removal, EKG interpretation for chest pain triage, joint injection for acute injury (when scope of practice permits), simple suture removal, simple cast/splint application
- 3-8 occupational health visits — work injury first-report with mechanism of injury narrative and work status determination, DOT CMV driver medical exams (Form MCSA-5875), pre-employment physicals, drug screen collections, return-to-work clearances after injury or illness, FAA airman medical certification touchpoints (when staffed by AME)
- 2-5 sports/school physical visits — AAP/AHA preparticipation physical with cardiac screening (PPE-5 monograph 14-element history and physical), school physicals
- Multi-purpose visits — vaccinations (flu, COVID, Tdap, HepB, HPV, MMR), travel medicine consultations and immunizations, simple wound care follow-ups, suture/staple removal, post-op evaluations sent over by surgical practices, medication refills for established care patients between PCP visits
Across this volume and breadth, the documentation burden is significant — and unique because the documentation must support multiple downstream uses simultaneously (medical record, billing, work-comp claim, DOT certification, school clearance, sports clearance, follow-up coordination, ED transfer summary).
What General-Purpose AI Scribes Miss in Urgent Care
Most AI medical scribes are tuned for the 15-minute primary care encounter — HPI, focused exam, MDM, plan. Urgent care documentation breaks general-purpose scribes in specific ways:
- Procedural CPT capture is high-volume. Urgent care providers commonly perform multiple procedures per shift. Documentation must support correct CPT capture: simple laceration repair (12001-12007 scalp/neck/axillae/external genitalia/trunk/extremities by length; 12011-12018 face/ear/eyelids/nose/lips/mucous membranes by length); intermediate laceration repair requiring layered closure (12031-12057); complex laceration repair requiring more than layered closure or extensive undermining (13100-13160); splinting (e.g., 29105 long-arm, 29125/29126 short-arm static/dynamic, 29130/29131 finger static/dynamic, 29515 short-leg, 29505 long-leg); casting (e.g., 29065 shoulder-to-hand spica, 29075 elbow-to-finger long-arm, 29085 hand/lower-forearm short-arm, 29086 finger cast, 29345/29355 long-leg, 29405/29425 short-leg); abscess I&D (10060 simple, 10061 complex/multiple, 10080/10081 pilonidal cyst); foreign body removal from skin/subcutaneous tissue (10120 simple, 10121 complex). Foreign body removal from the eye, ear canal, or nose uses separate code families (e.g., conjunctival/corneal FB 65205-65222; external auditory canal FB 69200/69205; intranasal FB 30300) which the documentation must distinguish. Final CPT/ICD-10 selection is the responsibility of the rendering provider and certified coders, not the AI scribe.
- Work-comp DWC documentation has state-specific forms. California requires DWC-1 (Employee's Claim Form) and DWC-PR-2 (Primary Treating Physician's Progress Report); Texas requires DWC-69 (Report of Medical Evaluation) and DWC-73 (Work Status Report); Florida requires DFS-F5-DWC-25 (Workers' Compensation Uniform Medical Treatment/Status Reporting Form); New York requires C-4 (Doctor's Initial Report) and C-4.2 (Progress Report). The AI must support state-specific work-comp documentation conventions including mechanism of injury detail, body parts injured, work-relatedness assessment, work status (full duty, modified with specific restrictions, off-work), expected duration, and treatment plan.
- DOT CMV driver medical examination is a 4-page form with specific findings. FMCSA Form MCSA-5875 (Medical Examination Report Form for Commercial Driver Fitness Determination) requires documentation of medical history (insulin-treated diabetes, hypertension status, cardiac history, sleep apnea, vision/hearing acuity, neurologic conditions, medications, drug/alcohol use, mental health), examination findings (vision 20/40 each eye and 70-degree field, hearing forced whisper at 5 feet, BP and pulse, urinalysis result for protein/glucose/blood/specific gravity), and certification decision (certified for 2 years, 1 year, 6 months, 3 months, or denied with specific reason). The AI must support this structured documentation.
- Sports physical and PPE-5 monograph 14-element screening. AAP/AHA preparticipation physical examination with personal history (chest pain or syncope with exertion, syncope or near-syncope unprovoked, excessive dyspnea or fatigue with exercise, prior heart murmur or hypertension, prior restriction from sports), family history (premature death before age 50 attributed to heart disease, disability from heart disease in close relative under 50, hypertrophic or dilated cardiomyopathy, long QT syndrome or arrhythmias, Marfan syndrome), and physical examination (cardiac auscultation supine and standing, pulses, blood pressure, Marfan habitus). The 14-element screening is documented in PPE-5 monograph format.
- Disposition documentation with EMTALA awareness. Urgent care providers screen patients who could potentially need ED-level care. EMTALA (Emergency Medical Treatment and Active Labor Act) applies to hospital-affiliated urgent cares and to all hospital-based emergency departments — but freestanding urgent cares without hospital affiliation are not directly subject to EMTALA. Disposition documentation must clearly establish whether the visit is appropriate for urgent care vs requires ED transfer with documented MSE-equivalent screening when transfer is appropriate.
- Antibiotic stewardship documentation. CDC Core Elements of Outpatient Antibiotic Stewardship require documentation of clinical justification for antibiotic prescriptions in conditions where antibiotic prescribing has high inappropriate-use rates — viral URI, viral pharyngitis with negative strep RADT, bronchitis, sinusitis (with duration justification for AOM bacterial diagnosis after 10 days or worsening course), conjunctivitis. The AI should support justification documentation when antibiotics are prescribed.
- Throughput timing. Urgent care documentation must complete in under 4 minutes per visit to maintain provider throughput at 4-6 visits per hour. A general-purpose AI scribe that produces a 4-minute note for a 7-minute encounter loses the time advantage urgent care needs.
The Multi-Purpose Documentation Product
Urgent care notes serve more downstream uses than typical primary care notes:
- Medical record — for continuity of care if the patient's PCP wants the record
- Insurance billing — supporting the E&M code (99202-99205 new / 99212-99215 established) and any procedure codes
- Work-comp claim — when the visit is related to work injury, the documentation goes to the employer's work-comp insurance carrier
- DOT certification record — for CMV driver medical exams, retained for 3 years per FMCSA requirements
- Sports/school clearance — the physical form returned to the patient and school/team
- Pre-employment record — retained by the employer
- ED transfer summary — when the patient is transferred to an ED
- Specialty referral packet — when the patient is referred to ortho, surgery, GI, cardiology
- Drug screen result documentation — for pre-employment, post-incident, or random drug screens
A general-purpose AI scribe that produces only the medical record narrative requires the urgent care provider to manually generate each downstream document — defeating much of the time-saving benefit.
Quick Comparison — Top AI Scribes for Urgent Care
| Rank | Tool | Price | UC-Specific | EHR Integration | Best For |
|---|---|---|---|---|---|
| 1 | DeepCura | $129/mo | Custom UC + procedural + work-comp templates | 9 EHRs (custom mapping) | Best Overall |
| 2 | Freed AI | $39-$104/mo | Generic SOAP, manual UC adaptation | Browser scrape (Premier) | Solo UC provider |
| 3 | Abridge AI | Custom enterprise | Hospital UC enterprise focus | Epic deep | Hospital UC |
| 4 | Heidi Health | $0-$99/mo | Generic templates, UC-adaptable | Limited write-back | Free tier trial |
| 5 | Suki AI | ~$199/mo | Voice-first ambient + dictation | Epic, Cerner, athena | Voice-first |
| 6 | DeepScribe | ~$199/mo | Customizable templates | Custom builds | Customization |
For a broader cross-specialty comparison, see our Best AI Medical Scribes in 2026 ranking. For emergency medicine tool selection, see our best AI scribe for emergency medicine guide.
What to Look For in an Urgent Care AI Scribe
Urgent care documentation requires breadth, procedural depth, and regulatory form support. Before choosing a tool, evaluate it against these eight criteria:
1. Acute Presentation Differential Generation. The AI must support broad-and-fast differential diagnosis across body systems and acuity levels — chest pain workup, abdominal pain workup, headache workup, dyspnea workup, syncope workup — with red flag screening and disposition reasoning.
2. Procedural CPT Capture. Laceration repair coding by length, anatomic region, and complexity (simple/intermediate/complex); splinting and casting coding by anatomic region and material; abscess I&D coding by complexity; foreign body removal coding; nail procedures; joint injection coding when in scope.
3. Work-Comp DWC Documentation. State-specific work-comp form support (California DWC-1/DWC-PR-2, Texas DWC-69/DWC-73, Florida DFS-F5-DWC-25, New York C-4/C-4.2) with mechanism of injury detail, work-relatedness assessment, work status determination with specific restrictions, expected duration, and treatment plan.
4. DOT CMV Driver Medical Examination. FMCSA Form MCSA-5875 support with structured medical history, examination findings, and certification decision documentation.
5. Sports/School Physical and PPE-5 Monograph Screening. AAP/AHA preparticipation physical with 14-element personal/family/physical screening, school physical templates, and pre-employment physical examination structures.
6. Antibiotic Stewardship Justification. CDC Core Elements antibiotic stewardship justification documentation when antibiotics are prescribed for high-inappropriate-use conditions (viral URI, viral pharyngitis, bronchitis, sinusitis).
7. Disposition Documentation with EMTALA Awareness. Clear documentation of treat-and-release, transfer-to-ED, admit, or follow-up disposition with appropriate MSE-equivalent screening when ED transfer is appropriate.
8. EHR Integration with Urgent Care PMS. Bidirectional integration with urgent-care-specific PMS (DocuTAP/Experity, Practice Velocity, eClinicalWorks UC, athenahealth, AdvancedMD, NextGen, Greenway). UC-specific PMS often have features that general EHRs lack (queue management, walk-in workflow, occupational health module).
Detailed Reviews
1. DeepCura — Best Overall for Urgent Care Documentation
DeepCura is a customizable clinical AI platform that combines ambient scribing, clinical decision support, evidence search, practice automation, and bidirectional EHR integration — $129/month with unlimited notes. For urgent care providers — single-site solo, multi-site groups, hospital-affiliated UCs outside the largest enterprise systems, and occupational medicine clinics — DeepCura's customizable templates and unlimited per-user notes deliver the strongest fit because urgent care documentation breadth and procedural/regulatory depth requires structural support that no off-the-shelf scribe ships with by default.
For urgent care providers, the key differentiator is template breadth and procedural capture depth. DeepCura's custom template builder lets practice leads encode urgent-care-specific templates: a general acute visit template with chief complaint, focused HPI with red flag screening, focused exam, results integration (RADT, UA, EKG, point-of-care glucose), differential and MDM, treatment, antibiotic stewardship justification when applicable, and disposition with follow-up; a procedural visit template with procedure name, indication, anatomy, technique (anesthesia type, suture material and size, layers closed for laceration; immobilization position and material for splint/cast; technique for I&D), CPT code with appropriate modifiers, and post-procedure instructions; a work-comp visit template with state-specific work-comp form support, mechanism of injury, work-relatedness assessment, work status with specific restrictions, expected duration, and treatment plan; a DOT CMV driver medical exam template with FMCSA Form MCSA-5875 structure; sports/school physical templates with PPE-5 monograph screening; pre-employment physical templates; drug screen documentation templates.
CDS Mode (3 credits per encounter) generates clinical decision support — particularly valuable for the chest pain visit requiring HEART score reasoning and disposition decision; the abdominal pain visit requiring surgical vs medical differential and red flag screening; the headache visit requiring secondary headache rule-out; the syncope visit requiring San Francisco Syncope Rule or Canadian Syncope Risk Score reasoning; and the work-comp visit requiring causation and apportionment reasoning.
DeepEvidentia — DeepCura's evidence search engine — pulls from PubMed, ACEP urgent care references, AAUCM (American Academy of Urgent Care Medicine) clinical pearls, IDSA antimicrobial guidelines, CDC Core Elements antibiotic stewardship references, FMCSA medical examiner handbook, AAP/AHA PPE-5 monograph, OSHA occupational health resources, and state work-comp medical guidelines. Useful for urgent care providers managing the breadth of presentations across regulatory and clinical domains.
Strengths:
- Custom templates per visit type (acute medical, procedural, work-comp, DOT, sports/school physical, pre-employment, drug screen) with urgent care conventions
- Procedural CPT capture for laceration repair, splinting, casting, abscess I&D, foreign body removal, nail procedures, joint injections
- State-specific work-comp DWC documentation support
- DOT CMV driver medical exam (FMCSA Form MCSA-5875) structured documentation
- Sports/school physical PPE-5 monograph screening
- Antibiotic stewardship justification documentation
- AI receptionist for after-hours triage and walk-in queue management — particularly valuable for urgent care
- Multiple AI engines matched to documentation complexity (1-15 credits)
- Unlimited notes per provider on all plans
- Bidirectional integration with urgent-care PMS (Experity/DocuTAP via integration partner work) and major EHRs (Epic, athenahealth, AdvancedMD, eClinicalWorks)
Limitations:
- Custom template builder requires meaningful initial setup (15-20 hours per practice to encode UC + procedural + work-comp + DOT + sports physical templates)
- Native integration with urgent-care-specific PMS (Experity, Practice Velocity) requires verifying integration depth — some integrations are bidirectional API, others are clipboard or browser-extension
- Multi-state practices with varying work-comp forms require state-specific template configuration
Pricing: $129/month per provider — all features included. Free trial available, no credit card required.
Verdict: DeepCura is the strongest choice for urgent care providers across single-site solo, multi-site group, hospital-affiliated UC, and occupational medicine settings. The flexibility cost is upfront setup time, but the per-user pricing and unlimited notes make it economically viable across UC scale.
DeepCura: Customizable AI Scribe for Urgent Care
UC visit templates, procedural CPT capture (laceration, splint/cast, I&D), work-comp DWC documentation, DOT exam (MCSA-5875), and sports physicals — $129/mo. Start your free trial.
+1 (415) 549-1829Available 24/7 · Set up in seconds · No credit card required
2. Freed AI — Best for Solo Urgent Care Provider
Freed AI is the most accessible ambient scribe for solo urgent care providers. The product is built around the conventional outpatient encounter and produces SOAP-format notes by default. For solo UC providers and small group UC practices running 25-40 patients per day, Freed at $79-$104/month with unlimited notes is one of the most cost-effective ambient scribes on the market.
The Premier tier at $104/month adds EHR push (browser-based scrape into the practice PMS) and ICD-10 coding suggestion. Procedural CPT capture, work-comp DWC documentation, DOT MCSA-5875, and sports physical PPE-5 screening require manual addition or post-editing.
Pricing: $39/month (Starter, 40 notes), $79/month (Core, unlimited), $104/month (Premier, unlimited + EHR push + ICD-10).
Verdict: Best for solo UC providers and small group UC practices who want fast ambient capture at the lowest defensible price point and are willing to invest in post-editing for UC-specific documentation. Read our Freed AI review.
3. Abridge AI — Best for Hospital-Affiliated Urgent Care
Abridge has emerged as the leading enterprise AI scribe for large health systems, with deployments at multiple major academic medical centers. For hospital-affiliated urgent cares within larger health systems on Epic, Abridge offers consistent infrastructure across the medicine service and the broader clinical team including UC.
The limitation is access — Abridge is enterprise-only and not available to freestanding urgent cares, multi-site UC chains outside the largest health systems, or independent UC providers. Pricing is custom (per-provider per-month with multi-year contracts).
Pricing: Custom enterprise contracts. Multi-year minimum.
Verdict: Best for hospital-affiliated urgent cares within enterprise health systems with Epic deep integration requirements. Read our Abridge AI review.
4. Heidi Health — Best Free Tier for Urgent Care Trial
Heidi Health offers a usable free tier (limited notes per month) that lets individual UC providers test ambient AI documentation at zero cost. Heidi has multi-specialty templates available and adapts to urgent care workflows with custom configuration.
US urgent care conventions (work-comp DWC, DOT MCSA-5875, US-specific sports physical forms, US antibiotic stewardship) require manual configuration on Heidi. PMS integration is limited (clipboard or email).
Pricing: Free tier (limited notes), Pro tier roughly $129/month, enterprise tier higher.
Verdict: Best for individual UC providers who want to test ambient AI documentation at zero cost before committing to a paid tool. Read our Heidi Health review.
5. Suki AI — Best Voice-First Urgent Care Tool
Suki AI offers a voice-first ambient and dictation product. For UC providers who prefer voice command over passive ambient capture (procedural rooms with motion and noise, multiple-patient throughput where ambient capture in one room interferes with capture in the next room), Suki provides a workable interaction model.
Suki's strengths are EHR integration depth (Epic, Cerner, athenahealth — though most freestanding UC chains do not run on these EHRs), the voice-first paradigm, and a mature commercial deployment record. Limitations for urgent care: Suki's primary focus is conventional physician/APP rather than UC-specific procedural and regulatory documentation, and CPT capture / work-comp DWC / DOT MCSA-5875 structure requires custom configuration.
Pricing: Approximately $199/month per user.
Verdict: Best for UC settings where voice-first dictation fits the workflow better than ambient capture, particularly hospital-affiliated UCs already using Epic or Cerner.
6. DeepScribe — Best for Customizable Urgent Care Templates
DeepScribe offers customizable AI scribe templates with deeper specialty configuration than off-the-shelf consumer-grade tools. For UC practices with internal template-building resources and willingness to invest in custom configuration, DeepScribe can produce UC-specific templates with procedural CPT capture, work-comp DWC support, and regulatory exam documentation.
Trade-off is price — DeepScribe is approximately $199/month per provider, roughly 50% higher than DeepCura at the same custom-template tier. DeepScribe also lacks DeepCura's bundled CDS, evidence search, and AI receptionist features valuable to UC throughput.
Pricing: Approximately $199/month per provider.
Verdict: Best for UC practices willing to pay a premium for custom-template ambient capture without the broader DeepCura platform features. Read our DeepScribe review.
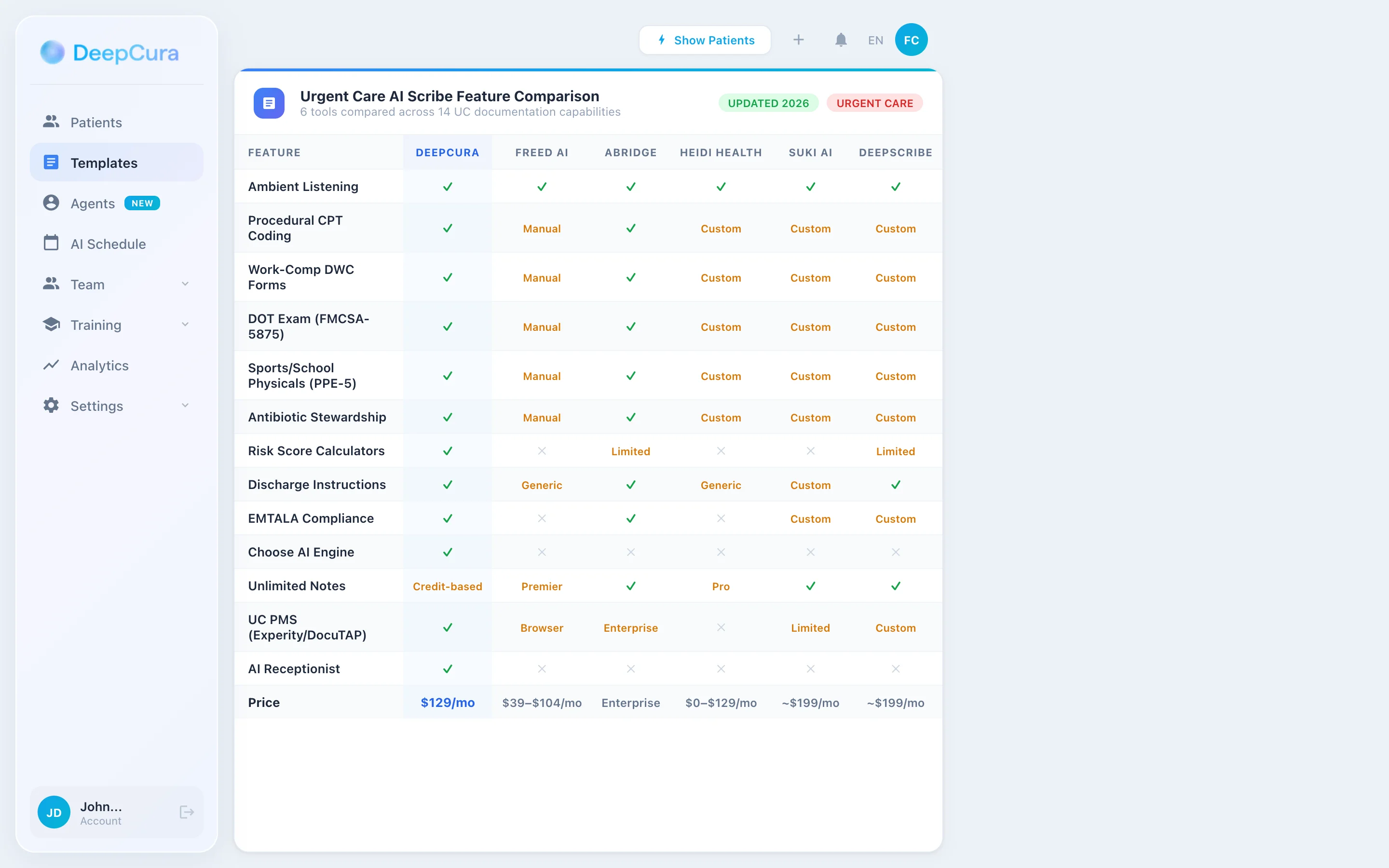
Head-to-Head — Urgent Care Documentation Features
| Feature | DeepCura | Freed | Abridge | Heidi | Suki | DeepScribe |
|---|---|---|---|---|---|---|
| Acute Presentation Differential | ✓ | Generic | ✓ Enterprise | Custom | Custom | ✓ Custom |
| Laceration Repair CPT (12001-13160) | ✓ | Manual | ✓ Enterprise | Custom | Custom | ✓ Custom |
| Splinting CPT (29105-29515) | ✓ | Manual | ✓ Enterprise | Custom | Custom | ✓ Custom |
| Casting CPT (29065-29086) | ✓ | Manual | ✓ Enterprise | Custom | Custom | ✓ Custom |
| Abscess I&D CPT (10060-10081) | ✓ | Manual | ✓ Enterprise | Custom | Custom | ✓ Custom |
| Work-Comp DWC (state-specific) | ✓ | Manual | ✓ Enterprise | Custom | Custom | ✓ Custom |
| DOT CMV Exam (MCSA-5875) | ✓ Custom | Manual | ✓ Enterprise | Custom | Custom | ✓ Custom |
| Sports/School Physical (PPE-5) | ✓ Custom | Manual | ✓ Enterprise | Custom | Custom | ✓ Custom |
| Antibiotic Stewardship Justification | ✓ | Manual | ✓ Enterprise | Custom | Custom | ✓ Custom |
| Disposition / EMTALA Awareness | ✓ | Generic | ✓ Enterprise | Custom | Custom | ✓ Custom |
| AI Receptionist (queue management) | ✓ | ✗ | ✗ | ✗ | ✗ | ✗ |
| Clinical Decision Support | ✓ (CDS Mode) | ✗ | Limited | ✗ | ✗ | Limited |
| EHR / UC PMS Bidirectional | 9 EHRs + custom | Browser scrape | Epic deep | Limited | Epic/Cerner/athena | Custom builds |
| Price | $129/mo all features | $39-$104/mo | Enterprise custom | $0-$99/mo | ~$199/mo | ~$199/mo |
Urgent Care Workflow with DeepCura
DeepCura's tiered credit system lets UC providers match AI resources to documentation complexity — fast for routine acute visits, deeper for procedural and regulatory documentation.
Routine Acute Visit (1 Credit) — Viral URI, Strep, UTI, Otitis, Simple MSK
For the high-volume routine acute visit — viral URI with negative strep RADT, simple UTI with positive UA, otitis media, conjunctivitis, simple ankle sprain without fracture suspicion — the 1-credit model generates a complete UC SOAP note in under 20 seconds. Speed-optimized for the UC provider running 4-6 visits per hour where every saved minute compounds across the shift.
Procedural and Work-Comp Visit (3 Credits CDS) — Laceration Repair, Splint, Cast, Work Injury
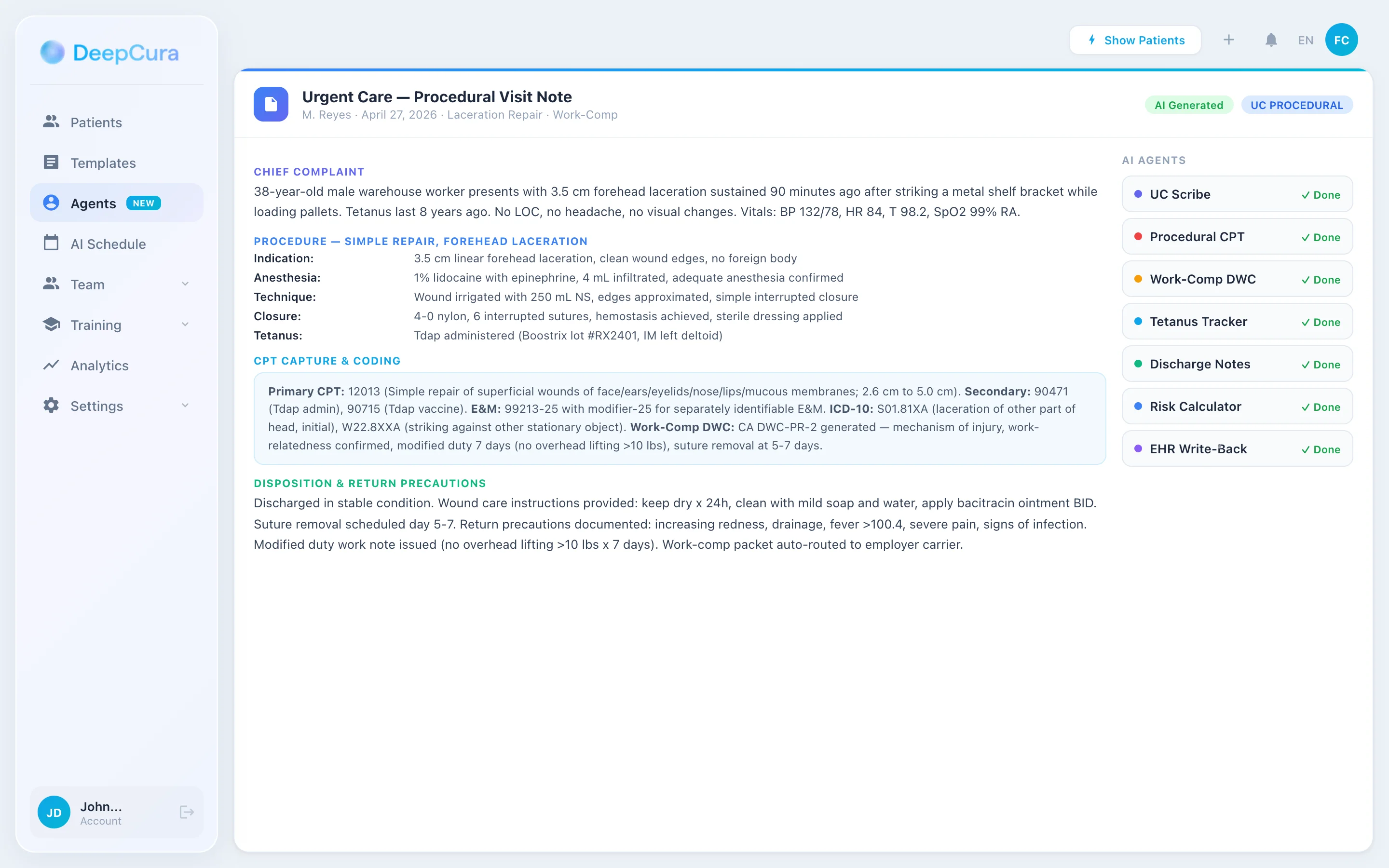
For procedural visits with documentation depth requirements — laceration repair with anatomic region, length, depth, layers closed, suture material, repair complexity, post-procedure instructions, and CPT capture; splinting or casting with indication, anatomy, immobilization position, materials, and CPT capture; abscess I&D with packing material and follow-up instructions — and for work-comp visits with state-specific DWC documentation, mechanism of injury detail, work-relatedness assessment, work status determination, and treatment plan — CDS Mode generates the structured procedural and regulatory documentation.
Complex Multi-System and DOT/Sports Physical (15 Credits) — DOT MCSA-5875, Sports PPE-5, Complex Acute, ED Transfer
For DOT CMV driver medical examination with full FMCSA Form MCSA-5875 structure, sports physical with PPE-5 monograph 14-element screening, complex multi-system acute presentations requiring detailed differential reasoning, and ED transfer summaries with full handoff narrative — the maximum-depth model produces the comprehensive narrative that supports both the regulatory document and the medical record.
From Walk-In to Documentation in Real Time
DeepCura templates for acute visits, procedures (laceration/splint/cast/I&D), work-comp DWC, DOT MCSA-5875, and sports physicals — $129/mo. Start your free trial.
+1 (415) 549-1829Available 24/7 · Set up in seconds · No credit card required
Clinical Decision Support and Evidence Search for Urgent Care
CDS Mode outputs are documentation-aid suggestions for clinician review. They are not diagnoses, treatment recommendations, or substitutes for clinical judgment. Disposition prompts (including any reference to ED transfer) are documentation aids; the clinician retains full responsibility for triage, EMTALA compliance where applicable, and disposition decisions. DeepCura is not an FDA-cleared medical device.
CDS Mode — Decision Support for Acute Presentations
UC providers manage broad acute presentations where differential and disposition reasoning matter. CDS Mode provides decision support for:
- Chest pain triage — HEART score (History, EKG, Age, Risk factors, Troponin) for ED-vs-discharge decision; PERC rule for low-risk PE; Wells score for higher-risk PE with d-dimer or CTPA decision
- Abdominal pain workup — surgical vs medical differential; red flag screening (peritoneal signs, severe pain disproportion to exam, hemodynamic instability, persistent vomiting, GI bleeding)
- Headache differential — primary (migraine, tension, cluster) vs secondary (SAH, meningitis, temporal arteritis, stroke) with red flag screening (sudden severe onset, focal neurologic deficit, fever with stiff neck, age >50 with new headache, immunocompromised)
- Syncope risk stratification — San Francisco Syncope Rule, Canadian Syncope Risk Score for ED-vs-discharge decision
- Sore throat with cough vs without cough — Centor criteria modified McIsaac score for strep RADT necessity vs viral diagnosis
- Antibiotic stewardship reasoning — when does sinusitis warrant antibiotics (10+ days symptoms or worsening course), when does AOM warrant immediate antibiotics vs watchful waiting (age, severity, otorrhea, bilateral disease)
For a 38-year-old man presenting with sudden onset severe chest pain, diaphoresis, and shortness of breath, CDS Mode flags: differential considerations (ACS — STEMI vs NSTEMI rule out; PE — Wells score and PERC; aortic dissection — pulse symmetry and chest X-ray; pneumothorax; pneumonia; MSK), HEART score components for ACS risk, immediate workup recommendations (EKG, troponin POC if available, CXR), disposition reasoning (most likely requires ED transfer for higher-acuity workup; document MSE-equivalent screening if hospital-affiliated UC, or transfer with comprehensive UC handoff if freestanding).
DeepEvidentia — Evidence at the Walk-In Visit for UC Providers
DeepEvidentia provides real-time access to PubMed, Cochrane, ACEP urgent care references, AAUCM clinical pearls, IDSA antimicrobial guidelines, CDC Core Elements antibiotic stewardship, FMCSA medical examiner handbook, AAP/AHA PPE-5 monograph, OSHA occupational health resources, and state work-comp medical guidelines.
Example queries UC providers actually ask:
- "HEART score interpretation and disposition cutoffs" — returns the HEART score 0-3 (low risk, discharge consideration with follow-up), 4-6 (moderate, likely ED for further workup), 7-10 (high, ED admission)
- "IDSA recommendations for sinusitis antibiotic timing" — returns the 10-day or worsening course threshold for antibiotic initiation
- "Centor criteria for strep pharyngitis" — returns Centor and McIsaac modified criteria with RADT vs no testing thresholds
- "Acute otitis media in adults — antibiotic vs watchful waiting" — returns IDSA/AAFP recommendations
- "FMCSA insulin-treated diabetes commercial driver certification" — returns the ITDM exemption pathway and certification requirements
- "California work-comp DWC-PR-2 reporting requirements" — returns DWC reporting timelines and content requirements
- "Sports physical sudden cardiac death screening — Marfan habitus assessment" — returns PPE-5 monograph cardiac screening elements
For UC providers managing the breadth of acute and regulatory documentation, evidence access at the visit reduces friction in clinical decision-making.
Pricing Comparison
| Tool | Monthly | Note Limit | UC-Specific | Best Plan |
|---|---|---|---|---|
| DeepCura | $129/mo | Unlimited | ✓ Custom UC + procedural + work-comp | Single plan, all features |
| Freed AI | $39-$104/mo | 40-unlimited | Manual | Premier ($104) |
| Abridge AI | Enterprise custom | Enterprise | ✓ | Enterprise contract |
| Heidi Health | $0-$99/mo | Free tier limited | Custom | Free or Pro |
| Suki AI | ~$199/mo | Unlimited | Custom | Pro tier |
| DeepScribe | ~$199/mo | Unlimited | ✓ Custom | Custom-built tier |
See DeepCura in Action
Watch how DeepCura handles the full urgent care workflow — acute presentations with differential reasoning, procedural CPT capture (laceration repair, splinting, casting, abscess I&D), work-comp DWC documentation, DOT CMV driver medical exam, sports/school physicals, and antibiotic stewardship justification.

Frequently Asked Questions
What is the best AI scribe for urgent care?
DeepCura is the strongest cross-functional choice for urgent care providers across single-site solo, multi-site group, hospital-affiliated UC outside the largest enterprise systems, and occupational medicine clinics. Customizable templates support acute medical visits, procedural CPT capture (laceration repair, splinting, casting, abscess I&D), work-comp DWC documentation, DOT CMV driver medical exams, sports/school physicals, and antibiotic stewardship justification. For hospital-affiliated UCs in enterprise health systems on Epic, Abridge AI is the enterprise leader. For solo UC providers prioritizing the lowest accessible price, Freed AI Premier at $104/month is also viable.
Do AI scribes capture procedural CPT codes for laceration repair, splinting, casting, and I&D?
DeepCura supports custom templates that capture procedural CPT codes — laceration repair (12001-13160 by length, anatomic region, and complexity), splinting (29105 long arm, 29125 short arm, 29130 finger, 29515 short leg), casting (29065 shoulder-to-hand, 29075 elbow-to-finger, 29085 hand-and-lower-forearm, 29086 finger), abscess I&D (10060 simple, 10061 complex, 10080/10081 pilonidal cyst), foreign body removal (10120 simple, 10121 complex), nail trephination (11740), nail avulsion (11730/11732). Enterprise tools support procedural CPT capture in their workflows. Consumer scribes require manual code addition.
Do AI scribes support state-specific work-comp DWC documentation (California, Texas, Florida, New York)?
DeepCura supports custom templates for state-specific work-comp documentation — California DWC-1 / DWC-PR-2, Texas DWC-69 / DWC-73, Florida DFS-F5-DWC-25, New York C-4 / C-4.2 — with mechanism of injury detail, work-relatedness assessment, work status determination with specific restrictions, expected duration, and treatment plan. Other tools require manual state-specific work-comp documentation.
Can AI scribes structure DOT CMV driver medical exam documentation (FMCSA Form MCSA-5875)?
DeepCura supports a custom template for FMCSA Form MCSA-5875 (Medical Examination Report Form for Commercial Driver Fitness Determination) with structured medical history, examination findings (vision, hearing, BP, urinalysis), and certification decision documentation (2 years, 1 year, 6 months, 3 months, or denied with specific reason). The AI does not replace the certified medical examiner's clinical judgment but produces the structured documentation supporting the certification.
Do AI scribes support sports physical PPE-5 monograph screening?
DeepCura supports custom templates for AAP/AHA preparticipation physical examination with PPE-5 monograph 14-element screening (personal cardiac history, family premature cardiac death history, cardiac auscultation supine and standing, Marfan habitus assessment). Other tools require manual PPE-5 monograph documentation.
Can AI scribes support antibiotic stewardship justification for viral URI, sinusitis, and bronchitis?
DeepCura supports custom templates that prompt antibiotic stewardship justification documentation when antibiotics are prescribed for high-inappropriate-use conditions — viral URI, viral pharyngitis with negative strep RADT, bronchitis without bacterial features, sinusitis (with duration justification for antibiotic initiation after 10 days symptoms or worsening course). DeepEvidentia provides IDSA and AAFP evidence references at the visit.
Do AI scribes integrate with urgent-care-specific PMS (Experity/DocuTAP, Practice Velocity)?
DeepCura integrates with major urgent-care-specific PMS via custom field mapping; depth varies by PMS. Experity (formerly DocuTAP and Practice Velocity, merged 2019) integrations are typically API-based or browser-extension. Practices on UC-specific PMS should verify integration depth during evaluation.
How much do AI scribes for urgent care cost?
Solo-friendly options run $39-$130/month per provider (Freed $39-$104, Heidi Pro $99, DeepCura $129). DeepScribe and Suki are approximately $199/month. Enterprise tools (Abridge) for hospital-affiliated UCs are custom-priced with multi-year contracts. For most urgent care practices outside the largest hospital systems, the $99-$130/month accessible-price tier with DeepCura provides extensive urgent-care-specific template support.
Final Verdict
For urgent care practices, the choice comes down to four profiles:
Best overall: DeepCura at $129/month — customizable acute medical, procedural, work-comp, DOT, and sports physical templates with procedural CPT capture (laceration repair 12001-13160, splinting 29105-29515, casting 29065-29086, abscess I&D 10060-10081, foreign body removal 10120/10121, nail procedures 11730-11740), state-specific work-comp DWC documentation (California DWC-1/DWC-PR-2, Texas DWC-69/DWC-73, Florida DFS-F5-DWC-25, New York C-4/C-4.2), DOT CMV driver medical exam (FMCSA Form MCSA-5875), sports/school physical (PPE-5 monograph), antibiotic stewardship justification, and AI receptionist for after-hours triage. The strongest choice for urgent care practices outside the largest enterprise health systems.
Best for solo UC at lowest price: Freed AI Premier at $104/month — strong ambient capture quality with browser-based EHR push, suitable for solo UC providers and small group UC practices willing to invest in post-editing for UC-specific procedural and regulatory documentation. Lacks native CPT capture or work-comp DWC support but the ambient capture core is strong.
Best for hospital-affiliated UC enterprise: Abridge AI — enterprise-grade with deep Epic integration, multi-role/multi-specialty deployment, and the IT/security/legal frameworks that hospital-affiliated UCs in academic medical centers and large IDS/EDC organizations require.
Best for free-tier UC trial: Heidi Health — free tier (limited notes) lets individual UC providers test ambient AI documentation at zero cost.
For a broader cross-specialty comparison, see our Best AI Medical Scribes in 2026 ranking. For emergency medicine and family medicine tool selection, see our best AI scribe for emergency medicine and best AI scribe for family medicine guides. For practices needing after-hours triage and intake automation, see our Best AI Medical Receptionist guide. For free copy-paste clinical templates, see our SOAP note template reference. If you are evaluating EMRs alongside the scribe decision, see our best EMR for small practices ranking.
References
[1] American Academy of Urgent Care Medicine, "AAUCM Clinical Practice Pearls and Position Statements," AAUCM. aaucm.org
[2] American College of Emergency Physicians, "ACEP Clinical Policies and Urgent Care Resources," ACEP. acep.org/patient-care/policy-statements
[3] Federal Motor Carrier Safety Administration, "Medical Examiner Handbook and Form MCSA-5875 Medical Examination Report Form," FMCSA. fmcsa.dot.gov/medical
[4] American Medical Association, "Current Procedural Terminology (CPT) — Integumentary, Musculoskeletal Procedures (10000-29999)," CPT Professional Edition, 2026.
[5] Centers for Disease Control and Prevention, "Core Elements of Outpatient Antibiotic Stewardship," CDC. cdc.gov/antibiotic-use/community/improving-prescribing/core-elements
[6] American Academy of Pediatrics, American Heart Association, "Preparticipation Physical Evaluation Monograph (PPE-5)," 5th Edition, 2019. aap.org/preparticipation-physical-evaluation
[7] Six AJ, Backus BE, Kelder JC, "Chest pain in the emergency room: value of the HEART score," Netherlands Heart Journal, 16(6), 191-196, 2008. pubmed.ncbi.nlm.nih.gov/18665203
[8] Infectious Diseases Society of America, "IDSA Practice Guidelines for Sinusitis, Streptococcal Pharyngitis, and Acute Otitis Media," IDSA. idsociety.org/practice-guideline
[9] Centers for Medicare & Medicaid Services, "Emergency Medical Treatment and Active Labor Act (EMTALA) — Hospital Affiliated Urgent Care Considerations," CMS. cms.gov/regulations-and-guidance/legislation/emtala
[10] California Division of Workers' Compensation, "DWC Forms — DWC-1, DWC-PR-2, and Medical Treatment Reporting Requirements," California DIR. dir.ca.gov/dwc/forms
[11] Texas Department of Insurance Division of Workers' Compensation, "DWC-69 Report of Medical Evaluation and DWC-73 Work Status Report," TDI-DWC. tdi.texas.gov/wc/forms