U.S. physicians spend 5.9 hours of every clinical day on EHR documentation — more than the 4 hours they spend in direct patient care — plus approximately 1.4-1.8 hours of after-hours documentation time per Arndt 2017 and follow-on studies. That ratio of documentation to face-to-face time is the strongest single predictor of burnout in outpatient medicine, and it does not improve with experience or seniority. The AMA Physician Health Survey reports 51% of physicians experience burnout symptoms, with documentation burden cited more often than workload, compensation, or administrative overhead as the proximate cause.
We ranked 6 AI scribes on the criteria that matter most for physician documentation across primary care, internal medicine, pediatrics, geriatrics, and outpatient subspecialties:
- MDM documentation for E&M coding — does the AI structure Medical Decision Making to support 99202-99215 levels (straightforward / low / moderate / high) and capture the documented data reviewed, problems addressed, and risk of complications?
- HPI and ROS completeness — does it capture the 8 HPI elements and structure ROS by 14 systems for E&M level support?
- MIPS quality measure capture — does it document USPSTF Grade A/B screenings, AWV elements, CCM/TCM time tracking, and HCC-relevant chronic conditions for risk adjustment?
- EHR bidirectional integration — direct write-back to Epic, Cerner, athenahealth, eClinicalWorks, AdvancedMD, and other EHRs physicians actually use?
All products were evaluated in February-April 2026. Pricing reflects publicly available rates. Enterprise-priced products were assessed based on disclosed ranges and verified physician practice reports.
Disclosure & methodology. This comparison is published by DeepCura, which is included in the ranking. Pricing and feature claims for competitor products reflect publicly available information as of the evaluation period above and may change — verify directly with each vendor before procurement. This article is editorial commentary; it is not medical, legal, billing, or compliance advice. CPT® is a registered trademark of the American Medical Association. All other product names and trademarks are property of their respective owners; references are nominative and do not imply affiliation or endorsement.
Why Physicians Need an AI Scribe
The Documentation-to-Care Inversion
The Sinsky et al. study published in Annals of Internal Medicine measured what physicians actually do during a clinic day using direct observation of 57 physicians across 4 specialties. The finding that became the most-cited statistic in physician burnout literature: physicians spent 27% of office time on direct clinical face time with patients and 49.2% on EHR and desk work. The Arndt et al. follow-up using EHR event logs across 142 family physicians in Wisconsin found 5.9 hours per day in the EHR, including 1.4 hours after clinic hours from home. That 1.4-1.77 hour after-hours window is what physicians call "pajama time" — and it is the single strongest predictor of physician burnout, intent to leave practice, and reduced clinical hours per week.
The documentation-to-care inversion did not exist before EHR adoption. In paper-chart practice, physicians averaged 12-15 minutes of charting per encounter and finished notes at the end of clinic. EHR documentation in 2026 — with structured problem lists, ICD-10 specificity, MDM elements, ROS templates, smart-text, dot-phrases, billing codifiers, MIPS quality measure capture, and HCC risk adjustment coding — averages 16-21 minutes per encounter and routinely extends past midnight in the form of pajama time.
The cost of this inversion is measurable: physicians reporting more than 2 hours of after-hours documentation per day report substantially higher rates of leaving clinical practice (Mayo Clinic Proceedings, Shanafelt et al.). The American Medical Association now lists EHR documentation as the #1 driver of physician burnout in its annual survey, ahead of workload, compensation, and patient complexity.
What Physician AI Scribes Actually Need to Solve
Physician documentation is not just transcription. The encounter conversation needs to be transformed into a structured clinical note that supports five distinct downstream uses:
- Clinical communication — the note communicates the encounter to the patient, future clinicians, consultants, and the patient's other care team members.
- E&M coding and billing — the note must support the level coded (99202-99215 for outpatient E&M) through documented HPI elements, ROS systems, exam findings, and MDM complexity. CMS auditors and payor RAC contractors review notes specifically for E&M support.
- MIPS quality measures — eligible clinicians under MIPS Promoting Interoperability and Quality categories need documented evidence of preventive screenings (USPSTF Grade A/B), chronic condition management, advance care planning, depression screening (PHQ-2/PHQ-9), and dozens more eCQMs.
- HCC risk adjustment — for Medicare Advantage, ACO, and value-based contracts, documented chronic conditions drive the patient's RAF (Risk Adjustment Factor) score and per-member-per-month payment. ICD-10 specificity matters — "diabetes" is RAF-irrelevant, "diabetes with chronic kidney disease, stage 3" carries risk adjustment weight.
- Medicolegal defense — the note is the primary defense in malpractice cases. Documentation completeness (especially of differential diagnoses considered and patient education provided) is the most-cited deficiency in adverse-outcome reviews.
A documentation-only ambient scribe handles #1 well and #2 partially. The remaining three — MIPS quality, HCC risk adjustment, and structured medicolegal-grade documentation — require an AI that understands the coding and quality framework, not just the conversation.
The Specialist-Generalist Tradeoff in AI Scribe Selection
Physicians evaluating AI scribes confront a tradeoff that does not exist in most software categories: specialist depth versus generalist breadth. Specialist scribes (purpose-built for a single specialty — see our best AI scribe for emergency medicine and best AI scribe for psychiatry guides) handle one specialty's templates, jargon, and billing codes natively but break when applied to adjacent practice areas. Generalist scribes (Freed, DeepScribe, generic Ambience) work across specialties but lose accuracy on specialty-specific terminology and coding.
DeepCura's approach — customizable templates with specialty-aware prompting — splits the difference. A multi-specialty group practice can run primary care, behavioral health, and outpatient cardiology on one platform with templates tuned per provider. Health systems on Epic running 30+ subspecialties typically default to Nuance DAX Copilot for Epic-native generalist depth at the cost of $369+/month per provider.
For most independent physicians and small group practices, the right answer is a generalist scribe that handles the bulk of outpatient encounters well plus customization for the specific practice's high-volume note types (well visits, chronic disease follow-ups, acute problems) — making DeepCura, Freed, and DeepScribe the primary candidates and Nuance DAX the enterprise default.
Quick Comparison — Top AI Scribes for Physicians
| Rank | Tool | Price | MDM/E&M Support | EHR Integration | Best For |
|---|---|---|---|---|---|
| 1 | DeepCura | $129/mo | Structured MDM + 99202-99215 | 9 systems (native + browser-based push) | Best Overall |
| 2 | Freed AI | $39-$104/mo | Basic MDM, ICD-10 on Premier | Browser-based EHR push | Solo Physicians |
| 3 | Abridge AI | Enterprise | Strong MDM, EM-validated | Epic-native | Health Systems |
| 4 | Nuance DAX | $369+/mo | Epic-native MDM | 40+ EHRs | Epic Shops |
| 5 | DeepScribe | ~$99-$149/mo | Customizable MDM | Limited | Mid-Range Ambient |
| 6 | Ambience Healthcare | Enterprise | Strong, customizable | Enterprise | Large Health Systems |
For a broader cross-specialty comparison, see our Best AI Medical Scribes in 2026 ranking.
What to Look for in a Physician AI Scribe
CMS billing rules summarized in this article are for general background only. Verify against current CMS Medicare Learning Network articles, the CPT® manual, and your compliance officer before billing decisions.
Physician documentation has eight requirements that distinguish a useful AI scribe from a transcription tool:
1. Structured MDM Documentation. The AI must capture and structure the three MDM elements per CMS 2021 E&M guidelines: Number and Complexity of Problems Addressed (minimal / low / moderate / high), Amount and/or Complexity of Data Reviewed and Analyzed (minimal / limited / moderate / extensive), and Risk of Complications/Morbidity/Mortality (minimal / low / moderate / high). The combination determines the E&M level and affects accurate visit-level documentation. Scribes that produce a narrative paragraph without separating MDM elements force physicians to re-edit for billing support.
2. HPI 8-Element Capture. Location, quality, severity, duration, timing, context, modifying factors, and associated signs/symptoms — the 8 HPI elements that support level-of-service documentation. The AI should structure HPI to make all 8 visible to coding auditors without burying them in prose.
3. Comprehensive ROS by System. ROS is reviewed by 14 systems (Constitutional, Eyes, ENMT, Cardiovascular, Respiratory, Gastrointestinal, Genitourinary, Musculoskeletal, Integumentary, Neurological, Psychiatric, Endocrine, Hematologic/Lymphatic, Allergic/Immunologic). The number of systems reviewed contributes to E&M level support, and an AI that captures patient-volunteered review-of-systems content during the conversation (e.g., the patient mentioning fatigue, weight loss, or insomnia) routes those into the correct ROS system rather than dropping them in HPI.
4. ICD-10 Specificity and HCC Awareness. For Medicare Advantage, ACO, and value-based contracts, ICD-10 specificity drives RAF (Risk Adjustment Factor) score. "Diabetes mellitus" (E11.9) carries no HCC weight; "Diabetes mellitus type 2 with diabetic chronic kidney disease, stage 3a" (E11.22 + N18.31) carries HCC weight that increases per-member-per-month payment. The best AI scribes suggest the most specific ICD-10 code supported by the documented findings.
5. MIPS eCQM Capture. Eligible clinicians need documented evidence of preventive screenings, chronic condition management, depression screening, advance care planning, BMI/blood pressure/A1c control, and dozens of other electronic clinical quality measures. An AI that recognizes when the conversation contained content satisfying an eCQM (e.g., depression screening with PHQ-9, fall risk assessment, advance directive discussion) and structures it into the appropriate quality module reduces the burden of MIPS reporting.
6. Annual Wellness Visit (AWV) Element Tracking. The AWV (G0438 first / G0439 subsequent) requires specific documented elements: HRA (Health Risk Assessment), establishing/updating the medical and family history, list of current providers and suppliers, BP/height/weight/BMI, cognitive screening, depression screening, functional ability and safety screening, written prevention plan, and personalized health advice. Scribes that recognize the AWV format and structure findings into the required elements support the higher reimbursement code.
7. CCM and TCM Time Tracking. Chronic Care Management (99490 standard 20-minute, 99487 complex 60-minute) and Transitional Care Management (99495 14-day moderate / 99496 7-day high complexity) are time-based codes. The AI should capture the time spent on care coordination, patient and caregiver communication, medication reconciliation, and care plan updates — and structure that documentation to support the time-based code billed.
8. Bidirectional EHR Integration. Direct write-back to Epic, Cerner, athenahealth, eClinicalWorks, AdvancedMD, NextGen, OptiMantra, CharmHealth, and other physician EHRs. Without bidirectional integration, the AI generates a note that the physician copy-pastes into the EHR — eliminating most of the time savings.
Detailed Reviews
1. DeepCura — Best Overall for Physicians
DeepCura is a customizable clinical AI platform combining ambient scribing with clinical decision support, evidence search, practice automation, and bidirectional EHR integration — $129/month with unlimited notes. For physicians across primary care, internal medicine, pediatrics, geriatrics, and outpatient subspecialties, DeepCura's combination of structured MDM documentation, customizable templates, and CDS Mode produces a strong feature-to-cost ratio for full-spectrum primary and specialty care.
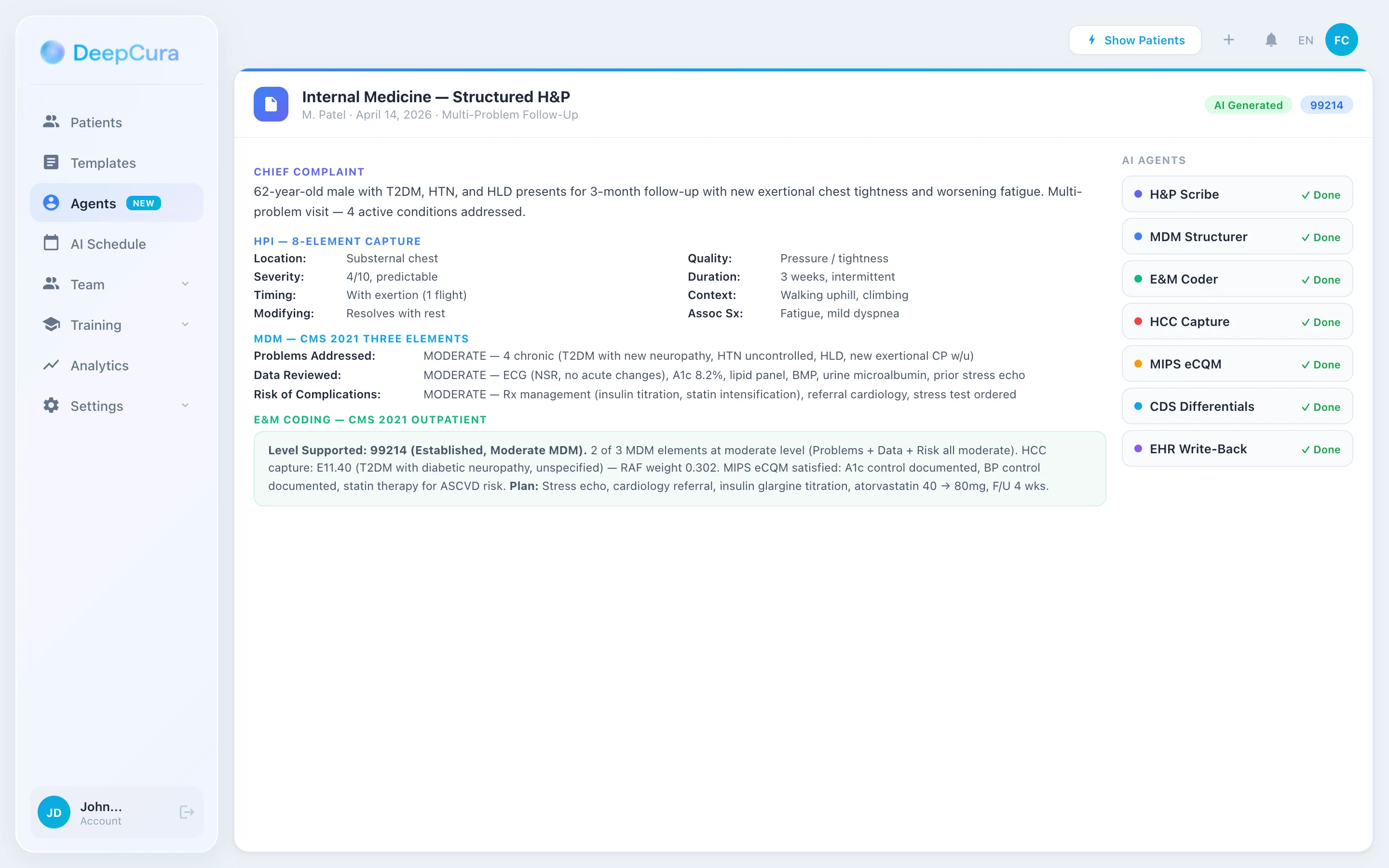
For physician documentation, DeepCura's key differentiators are MDM structuring and CDS Mode. The AI separates Medical Decision Making into the three CMS 2021 elements (Problems Addressed, Data Reviewed, Risk) so the documented support for E&M level is visible to coders and auditors without re-editing. CDS Mode, when activated (3 credits per note), generates differential diagnoses alongside the clinical note — useful for the broad-differential presentations that fill primary care (chest pain in adults, abdominal pain in adults, fatigue, headache, dizziness) where the documented differential is part of medicolegal defense.
DeepEvidentia — DeepCura's evidence search engine — pulls from PubMed, Google Scholar, USPSTF recommendations, FDA drug labels, and clinical guidelines mid-encounter. "USPSTF colorectal cancer screening recommendation for 45-year-olds" returns the Grade B recommendation with citation. "Metformin contraindication in eGFR <30" returns the FDA label guidance.
Strengths:
- Structured MDM documentation supporting 99202-99215 with three CMS 2021 elements visible
- HPI 8-element + ROS by 14 systems capture
- CDS Mode with differential diagnoses (3 credits per note)
- DeepEvidentia evidence search (PubMed, USPSTF, FDA, clinical guidelines)
- Customizable templates per specialty (FM/IM/peds/geriatrics/cardiology/etc.)
- Multiple AI engines matched to encounter complexity (1-15 credits)
- Native integrations with Epic, Cerner, athenahealth, AdvancedMD, and eClinicalWorks; additional EHRs supported via browser-based push (Veradigm, CharmHealth, OptiMantra)
- AI receptionist for after-hours triage and appointment scheduling
- Billing automation with E&M coding integrity checks
- Unlimited notes on all plans
Limitations:
- CDS Mode costs additional credits (3 per note vs. 1 for standard) — the ROI is positive for medicolegally-significant encounters but adds up across high-volume wellness visits
- Specialty-specific templates require initial setup time (typically 2-4 hours per high-volume note type to encode)
- HCC risk adjustment suggestion is automated but the physician must validate ICD-10 specificity
Pricing: $129/month per provider — all features included. Free trial available, no credit card required.
Verdict: DeepCura is the strongest choice for independent physicians and small group practices that want a single platform handling scribing, CDS, evidence search, and AI receptionist with structured MDM documentation built in. At $129/month with unlimited notes and 9-system EHR integration, it offers the most complete physician documentation solution at independent-practice pricing.
DeepCura: AI Scribe with Structured MDM and CDS
MDM elements visible for 99202-99215, CDS differentials, evidence search, and bidirectional EHR integration — $129/mo, unlimited notes. Start your free trial.
+1 (415) 549-1829Available 24/7 · Set up in seconds · No credit card required
2. Freed AI — Simplest Ambient for Solo Physicians
Freed AI is the cleanest, fastest ambient scribe for solo physicians who want documentation without complexity. Click record, see the encounter transcribed, get a structured SOAP note. The learning curve is measured in minutes rather than hours, and the tiered pricing is the most accessible in the market: $39/month for 40 notes on Starter, $79/month for unlimited on Core, and $104/month for unlimited with EHR push and ICD-10 coding on Premier.
For primary care physicians and outpatient internal medicine, Freed produces clean SOAP notes with adequate HPI and ROS structure. The MDM documentation is basic — narrative format rather than the three CMS 2021 elements separated for E&M coding support — so coders may need to re-review for level support, particularly on moderate-to-high complexity encounters. ICD-10 coding on Premier is helpful for problem list maintenance but does not consistently target HCC-relevant specificity for value-based contracts.
EHR integration is browser-based EHR push rather than native API write-back, which means notes are pushed via screen overlay rather than written to structured EHR fields. For Epic and Cerner shops with strict integration requirements, this is a meaningful limitation. For independent physicians on smaller EHRs (eClinicalWorks, AdvancedMD, NextGen) the browser-based push works adequately.
Pricing: $39/month (Starter, 40 notes), $79/month (Core, unlimited), $104/month (Premier, unlimited + EHR push + ICD-10).
Verdict: Best for solo physicians and small group practices that want dead-simple ambient documentation with the lowest learning curve. Not ideal for practices that need structured MDM for high-complexity coding, MIPS quality measure capture, or HCC risk adjustment optimization. Read our Freed AI review.
3. Abridge AI — Best for Health System Deployments
Abridge AI has built the strongest research-grade evidence base in the AI scribe market with peer-reviewed publications on documentation accuracy, physician satisfaction, and time savings across multiple health systems. That research base — combined with linked-evidence transparency (each note element traces back to a moment in the recording) — makes Abridge the natural choice for academic medical centers, integrated delivery networks, and health systems running formal clinical AI evaluation programs.
For physicians within Abridge-deployed systems, the documentation experience is strong. MDM is captured with appropriate structure for E&M coding, ROS coverage is comprehensive, and the linked-evidence feature reduces medicolegal anxiety because every clinical assertion in the note can be verified against the recorded conversation. Epic integration is well-developed and the platform is designed for enterprise security and compliance controls.
The constraint is procurement model. Abridge is enterprise-priced and not publicly disclosed, requires institutional procurement processes, and is generally not accessible to independent physicians or small group practices. For health systems on Epic with the procurement budget and timeline for enterprise AI deployment, Abridge is the strongest research-backed option.
Pricing: Enterprise custom — not publicly disclosed. Requires institutional procurement.
Verdict: Best for health systems and academic medical centers that want research-validated AI documentation with linked-evidence transparency and Epic-native enterprise deployment. Pricing and procurement requirements exclude independent physicians. Read our Abridge AI review.
4. Nuance DAX Copilot — Best for Epic Shops
Nuance DAX Copilot (Microsoft) has extensive Epic integration and compatibility with 40+ EHR systems — the broadest integration footprint of any AI scribe. For physicians in Epic-standardized health systems, DAX integrates into existing EHR workflows with minimal friction, supports Epic-native MDM templates, and benefits from Microsoft's enterprise security backing and long-term development investment.
DAX handles outpatient encounters across primary care, internal medicine, and most outpatient subspecialties through ambient listening and generates notes within Epic. Documentation quality is solid for general outpatient medicine. The platform is designed for enterprise deployment — implementation typically requires institutional IT engagement and a formal rollout plan.
The tradeoff is cost. DAX starts at $369/month per provider plus a $700 one-time implementation fee. For independent physicians and small group practices, that pricing is impractical compared to the $39-$129 range of generalist scribes. There is no clinical decision support or evidence search capability — DAX is a documentation tool, not a clinical reasoning platform.
Pricing: $369/month per provider (Solo/Group) + $700 one-time implementation. Enterprise volume discounts available.
Verdict: The default for Epic-standardized health systems and large multi-specialty groups with enterprise procurement budgets. The $369+ price point makes it impractical for independent physicians. See our Nuance DAX comparison.
5. DeepScribe — Mid-Range Ambient with Template Flexibility
DeepScribe offers ambient AI documentation with a customizable template engine that lets practice managers build SOAP, narrative, and structured note formats per specialty. The platform handles ambient capture reasonably well across primary care, internal medicine, and outpatient subspecialties, and the template flexibility accommodates practice-specific documentation requirements.
For physicians, DeepScribe's MDM documentation is adequate for routine outpatient coding but requires custom prompt engineering for the three-element CMS 2021 structure visible to coders. ICD-10 specificity and HCC risk adjustment awareness are not native — practices must validate these post-generation. EHR integration is more limited than DeepCura's 9-system bidirectional coverage or Nuance DAX's 40+ system compatibility, with most integrations relying on copy-paste or basic API push.
Pricing: Approximately $99-$149/month range. Custom enterprise pricing for larger practices.
Verdict: Solid mid-range ambient option for physicians and small group practices that want template flexibility and don't need specialty-specific tuning out of the box. Less feature-complete than DeepCura at similar pricing. Read our DeepScribe review.
6. Ambience Healthcare — Health System Focus
Ambience Healthcare targets large health system deployments with AutoScribe ambient documentation and Chart Awareness context engine. The platform is designed for enterprise-scale implementations with custom integrations tailored to institutional workflows and dedicated implementation support.
For physicians within Ambience-deployed health systems, the documentation experience offers strong context awareness — the Chart Awareness engine surfaces relevant prior encounters, problem list, medications, and labs during the current visit, which helps physicians on complex chronic care patients with extensive medical histories. Documentation quality across general outpatient medicine is competitive with Abridge and Nuance DAX.
The constraint is the same as Abridge: enterprise procurement, custom pricing, and institutional deployment requirements that exclude independent physicians and small group practices.
Pricing: Enterprise custom — requires institutional procurement.
Verdict: For large health systems with dedicated IT teams, enterprise procurement budgets, and the infrastructure to support custom AI implementations. Not accessible to independent physicians or small group practices. Read our Ambience Healthcare review.
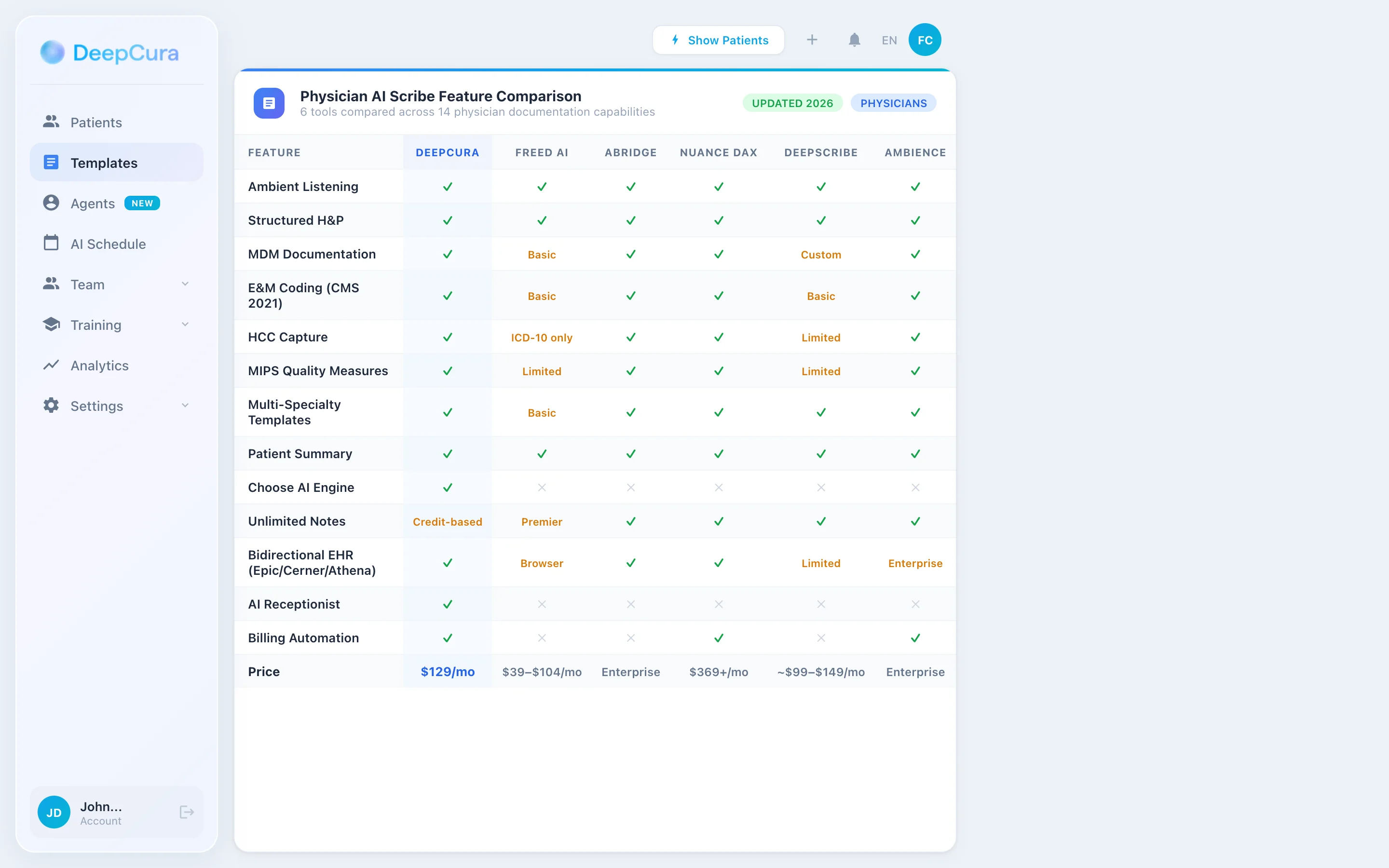
Head-to-Head — Physician Documentation Features
| Feature | DeepCura | Freed AI | Abridge | Nuance DAX | DeepScribe | Ambience |
|---|---|---|---|---|---|---|
| Ambient Listening | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Structured MDM (3 elements) | ✓ | Basic | ✓ | ✓ | Custom | ✓ |
| HPI 8-Element + ROS 14-System | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| E&M 99202-99215 Support | ✓ | Basic | ✓ | ✓ | Basic | ✓ |
| ICD-10 / HCC Awareness | ✓ | ICD-10 (Premier) | ✓ | ✓ | Limited | ✓ |
| MIPS eCQM Capture | ✓ | Limited | ✓ | ✓ | Limited | ✓ |
| AWV / CCM / TCM Templates | ✓ | Limited | ✓ | ✓ | Custom | ✓ |
| Clinical Decision Support | ✓ (differentials) | ✗ | ✗ | ✗ | ✗ | ✗ |
| Evidence Search | ✓ (DeepEvidentia) | ✗ | ✗ | ✗ | ✗ | ✗ |
| Choose AI Engine | ✓ | ✗ | ✗ | ✗ | ✗ | ✗ |
| Unlimited Notes | ✓ | Premier | ✓ | ✓ | ✓ | ✓ |
| Bidirectional EHR | ✓ (9 systems) | Browser-based EHR push | ✓ (Epic) | ✓ (40+) | Limited | Enterprise |
| AI Receptionist | ✓ | ✗ | ✗ | ✗ | ✗ | ✗ |
| Price | $129/mo | $39-$104/mo | Enterprise | $369+/mo | ~$99-$149/mo | Enterprise |
Physician Documentation Workflow with DeepCura
DeepCura's tiered credit system lets physicians match AI resources to encounter complexity — fast for routine well visits and follow-ups, deeper for complex chronic care and high-MDM presentations.
Routine Follow-Up (1 Credit) — Stable Chronic Disease, Medication Refills, AWV
For routine follow-up visits — well-controlled hypertension recheck, diabetes recheck with stable A1c, AWV (G0438/G0439), medication refills, low-acuity acute presentations (URI, simple UTI, allergic rhinitis) — the 1-credit model generates a structured SOAP note in under 30 seconds with HPI, ROS, exam, MDM, and plan completed. Speed-optimized for the high-volume routine day. No CDS overhead for encounters where the diagnosis is clinically obvious and MDM is straightforward or low.
Moderate Complexity (3 Credits CDS) — New Symptoms, Chronic Disease Worsening, Differential Workup
For moderate-MDM encounters — new chest pain in an adult, new abdominal pain with concerning features, worsening heart failure symptoms, diabetic patient with new neuropathy, new headache pattern, diagnostic workup of fatigue or unintentional weight loss — CDS Mode activates differential diagnosis generation alongside the SOAP note. The AI surfaces differential considerations the clinician may want to document (PE in chest pain with risk factors, malignancy in unintentional weight loss, ischemia in new exertional symptoms), validates that the documented workup addresses the differential, and structures MDM documentation so coders and clinicians can accurately assign the appropriate visit level.
High Complexity (15 Credits) — Multi-Problem Visits, New Diagnosis with Workup, Hospital Discharge Follow-Up
For high-MDM encounters — multi-problem visits with 4+ active conditions addressed, new diagnosis with extensive workup planned, hospital discharge follow-up with TCM (99495/99496), complex chronic care (99487 60-minute), suspected malignancy with referral coordination, high-risk medication initiation — the maximum-depth model produces comprehensive documentation with full MDM at high complexity, structured care coordination notes for TCM/CCM time tracking, and detailed differential diagnosis analysis where ambiguous presentations remain.
Match AI to Encounter Complexity
1 credit for routine follow-ups, 3 credits for CDS on moderate-MDM visits, 15 credits for high-complexity encounters — DeepCura scales documentation depth to match clinical complexity. Start your free trial.
+1 (415) 549-1829Available 24/7 · Set up in seconds · No credit card required
Clinical Decision Support and Evidence Search for Physicians
CDS Mode — Differentials for Medicolegal-Grade Documentation
CDS Mode outputs are documentation-aid suggestions for clinician review. They are not diagnostic or treatment recommendations. The clinician retains full responsibility for diagnosis, workup, and treatment decisions. DeepCura is not an FDA-cleared medical device.
Primary care, internal medicine, and outpatient subspecialty practice are full of broad-differential presentations where the documented differential is part of medicolegal defense. The chest pain workup in a 50-year-old smoker. The new headache pattern in a 65-year-old. The fatigue and weight loss workup. The new abdominal pain with red-flag features. The dizziness presentation that could be benign positional vertigo, or vestibular neuritis, or vertebrobasilar insufficiency, or Meniere's, or anxiety, or medication-induced.
CDS Mode activates differential diagnosis generation alongside the clinical note. For a 58-year-old presenting with new exertional chest pain, CDS Mode surfaces differential considerations the clinician may want to document such as acute coronary syndrome (ischemia rule-out), aortic dissection (in select presentations), pulmonary embolism (with risk factors), pneumothorax, esophageal pathology, and musculoskeletal etiologies. Suggested workup elements appear in the plan section for clinician review and modification, and the documented differential becomes part of the chart — protective in the rare adverse-outcome case where a missed diagnosis becomes a malpractice claim.
As of our February-April 2026 evaluation, DeepCura is the only product we reviewed that markets a CDS Mode with explicit differential generation as part of the standard documentation workflow. Freed, Abridge, Nuance DAX, DeepScribe, and Ambience are marketed primarily as documentation tools. DeepCura adds the clinical reasoning layer on top of documentation.
DeepEvidentia — Evidence at the Point of Care
DeepEvidentia provides real-time access to PubMed, Google Scholar, USPSTF Recommendation Statements, FDA drug labels, CDC ACIP immunization schedules, and major society guidelines (ACC/AHA, ADA, GOLD, KDIGO, AGA, USPSTF) directly within the documentation workflow.
Example queries physicians actually ask during outpatient encounters:
- "USPSTF colorectal cancer screening recommendation for adults 45-49" — returns Grade B recommendation with citation and rationale
- "ADA 2026 standards for SGLT2 initiation in type 2 diabetes" — surfaces ADA guidelines with eGFR thresholds and CV/renal benefit indications
- "2017 ACC/AHA hypertension diagnostic threshold (130/80 mmHg) for adults" — returns BP target with grade of recommendation
- "Metformin contraindication in eGFR less than 30" — returns FDA label guidance
- "Shingrix two-dose schedule for adults 50+" — returns CDC ACIP recommendation with dosing interval
For physicians who frequently encounter unfamiliar presentations, rare drug interactions, evolving guidelines, and quality-measure-relevant screening decisions, bedside evidence access transforms documentation time into clinical decision-making time.
Pricing Comparison
| Tool | Monthly | Note Limit | CDS | Best Plan |
|---|---|---|---|---|
| DeepCura | $129/mo | Unlimited | ✓ (3 credits/note) | Single plan, all features |
| Freed AI | $39-$104/mo | 40-unlimited | ✗ | Core ($79) or Premier ($104) |
| Abridge AI | Enterprise | Unlimited | ✗ | Custom health system pricing |
| Nuance DAX | $369+/mo | Unlimited | ✗ | Solo ($369) or Enterprise |
| DeepScribe | ~$99-$149/mo | Unlimited | ✗ | Standard plan |
| Ambience | Enterprise | Unlimited | ✗ | Custom health system pricing |
See DeepCura in Action
Watch how DeepCura handles the full physician workflow — ambient SOAP generation with structured MDM, CDS differentials, evidence search via DeepEvidentia, automated billing with E&M coding, and bidirectional EHR write-back.

Frequently Asked Questions
What is the best AI scribe for physicians in 2026?
DeepCura is the best overall AI scribe for independent physicians and small group practices in 2026 — at $129/month with unlimited notes, structured MDM documentation supporting 99202-99215, CDS Mode for differential diagnosis generation, evidence search via DeepEvidentia, and bidirectional EHR integration across 9 systems. For health systems on Epic with enterprise procurement budgets, Nuance DAX Copilot is the standard at $369+/month. For solo physicians who want the simplest ambient experience and are willing to do their own MDM editing, Freed AI at $39-$104/month is the most accessible entry point.
Do AI scribes support MDM documentation for E&M coding?
Quality varies significantly. The best AI scribes (DeepCura, Abridge, Nuance DAX) capture the three CMS 2021 MDM elements separately — Number and Complexity of Problems Addressed, Amount of Data Reviewed, and Risk of Complications — making the documented support for E&M level visible to coders and auditors. Freed AI and basic DeepScribe configurations produce narrative MDM that requires manual restructuring for high-complexity coding. For practices billing significant volumes of 99214 / 99215, MDM structure quality affects documentation completeness and coding accuracy.
Can AI scribes capture MIPS quality measures and HCC risk adjustment?
Partially. The strongest AI scribes recognize MIPS-relevant content during the encounter — depression screening with PHQ-9, fall risk assessment, advance care planning discussion, BMI/BP/A1c documentation, AWV elements — and route them into the appropriate quality module. HCC risk adjustment requires ICD-10 specificity (e.g., distinguishing E11.9 from E11.22 + N18.31), which DeepCura and Abridge support through specificity suggestions during documentation. No AI scribe replaces human coder review for value-based contract optimization, but the best tools front-load the documentation completeness needed.
Do AI scribes work with Epic, Cerner, athenahealth, eClinicalWorks, and AdvancedMD?
Yes, with varying integration depth. Nuance DAX has extensive Epic integration (40+ EHRs total). DeepCura offers bidirectional integration across 9 systems via FHIR R4 and EHR-specific APIs, including Epic, Cerner, athenahealth, eClinicalWorks, AdvancedMD, Veradigm, CharmHealth, and OptiMantra. Abridge has strong Epic integration designed for health system deployments. Freed AI uses browser-based EHR push rather than native API integration, which works adequately for smaller EHRs but lacks the structured-field write-back of native integrations.
How much do AI scribes for physicians cost?
Pricing ranges from $39/month to enterprise custom. Freed AI starts at $39/month (Core at $79, Premier at $104 with EHR push and ICD-10). DeepScribe costs approximately $99-$149/month. DeepCura is $129/month with unlimited notes, structured MDM, CDS, evidence search, and 9-system EHR integration. Nuance DAX starts at $369/month plus a $700 implementation fee. Abridge and Ambience require enterprise procurement with custom pricing. For most independent physicians, the $99-$129/month range offers the best feature-to-cost ratio.
Are AI scribes accurate for primary care multi-problem visits?
Modern AI scribes handle multi-problem visits well when the underlying note structure supports discrete problems with separate HPI, assessment, and plan sections per problem. DeepCura, Abridge, and Nuance DAX produce strong multi-problem documentation. Freed AI handles 2-3 problems well but can blur boundaries on 5+ problem visits typical of family medicine and geriatrics. For primary care practices with high-volume multi-problem days, evaluate scribe performance specifically on a 4-5 problem encounter during the trial period.
Can AI scribes document advance care planning, end-of-life discussions, and goals-of-care conversations?
Yes, and this is increasingly important for both MIPS quality measures and HCC risk adjustment. The advance care planning code (99497 first 30 minutes, 99498 each additional 30 minutes) requires documented evidence of the discussion, not just acknowledgment. The best AI scribes capture the substance of goals-of-care conversations — patient values, prognosis discussion, treatment preferences, designated decision-makers, advance directive status — and structure them to support the time-based code. DeepCura's CDS Mode also supports clinically-appropriate prompting for advance care planning in patients with serious illness.
What about HIPAA compliance, BAAs, and PHI handling?
All AI scribes in this comparison are HIPAA-compliant and offer Business Associate Agreements. The differences are in ambient recording handling, transcript retention policies, and de-identified data use. DeepCura, Abridge, Nuance DAX, and Ambience all support enterprise-grade HIPAA controls including BAA, audit logging, and configurable retention. Freed and DeepScribe offer BAAs; verify scope and tier requirements during procurement. Always review the BAA terms, transcript retention default, and AI training data use policies with your compliance officer before deployment.
Final Verdict
For physicians and physician groups, the choice comes down to three profiles:
Best overall: DeepCura at $129/month — structured MDM documentation supporting 99202-99215, CDS differentials, evidence search via DeepEvidentia, AI receptionist, customizable per-specialty templates, and unlimited notes. The strongest combination for independent physicians and small group practices that want a single platform handling scribing, CDS, and practice automation at independent-practice pricing.
Best simplest: Freed AI at $79-$104/month — dead-simple ambient documentation for solo physicians who want clean SOAP notes without the overhead of CDS, MIPS quality capture, or HCC optimization. The fastest learning curve in the AI scribe market, with a clean interface that stays out of the way.
Best enterprise: Nuance DAX Copilot at $369+/month — extensive Epic integration for health systems with enterprise procurement budgets and institutional standardization requirements. The default for Epic-standardized health systems where Epic compatibility and Microsoft enterprise support are non-negotiable.
For a broader cross-specialty comparison, see our Best AI Medical Scribes in 2026 ranking. For specialty-specific comparisons, see our best AI scribe for emergency medicine, best AI scribe for psychiatry, and best AI scribe for family medicine guides. For practices that need phone automation alongside documentation, see our Best AI Medical Receptionist guide. For clinical AI chat tools that support diagnostic reasoning, see Best ChatGPT for Doctors. For free copy-paste clinical note templates, see our SOAP note template guide. If you are choosing an EHR for a small practice, see our best EMR for small practices ranking.
References
[1] Sinsky CA, Colligan L, Li L, et al., "Allocation of Physician Time in Ambulatory Practice: A Time and Motion Study in 4 Specialties," Annals of Internal Medicine, 165(11), 753-760, 2016. acpjournals.org/doi/10.7326/M16-0961
[2] Arndt BG, Beasley JW, Watkinson MD, et al., "Tethered to the EHR: Primary Care Physician Workload Assessment Using EHR Event Log Data and Time-Motion Observations," Annals of Family Medicine, 15(5), 419-426, 2017. annfammed.org/content/15/5/419
[3] American Medical Association, "AMA Physician Health Survey 2024 — Burnout and Practice Sustainability," AMA. ama-assn.org/practice-management/physician-health
[4] Centers for Medicare & Medicaid Services, "Evaluation and Management Services Guide — CPT Codes 99202-99215 and 2021 MDM Documentation Guidelines," CMS.gov. cms.gov/medicare/payment/prospective-payment-systems
[5] Centers for Medicare & Medicaid Services, "MIPS Quality Performance Category and Electronic Clinical Quality Measures (eCQMs)," QPP.cms.gov. qpp.cms.gov/mips/quality-requirements
[6] U.S. Preventive Services Task Force, "USPSTF Recommendation Statements — Grade A and B Preventive Services," USPSTF. uspreventiveservicestaskforce.org
[7] Shanafelt TD, West CP, Sinsky C, et al., "Changes in Burnout and Satisfaction With Work-Life Integration in Physicians and the General US Working Population Between 2011 and 2020," Mayo Clinic Proceedings, 97(3), 491-506, 2022. mayoclinicproceedings.org
[8] Centers for Medicare & Medicaid Services, "Annual Wellness Visit (AWV) — G0438 First Visit and G0439 Subsequent Visits," CMS.gov. cms.gov/medicare/preventive-services
[9] Centers for Medicare & Medicaid Services, "Chronic Care Management Services — CPT 99490 and Complex CCM CPT 99487," CMS.gov. cms.gov/medicare/medicare-fee-for-service-payment/care-management
[10] U.S. Department of Health and Human Services, "HIPAA for Professionals — Business Associate Agreements," HHS.gov. hhs.gov/hipaa/for-professionals/business-associates
[11] DeepCura, "AI Medical Scribe Platform — Ambient Scribing, CDS, AI Receptionist, EHR Integration," DeepCura.com. deepcura.com