Many psychologists in independent practice spend a substantial portion of their week on documentation — psychological evaluations, integrated reports, neuropsychological assessments, treatment progress notes, and forensic narratives — and the long-form report is the single most time-consuming product in clinical psychology. Based on practitioner reports, a standard psychoeducational evaluation takes 8-12 hours of report writing alone after testing is complete; a neuropsychological evaluation runs 12-20 hours; a forensic competency-to-stand-trial evaluation can take 15-25 hours. Practitioners commonly report that report writing and integrated documentation contribute significantly to burnout.
We ranked 5 AI scribes on the criteria that matter most for psychologist documentation:
- Psychological testing report scaffolding — does the AI support the long-form integrated report (referral question, background, behavioral observations, test administration, results-by-domain, integrated formulation, diagnoses, recommendations) — not just a 50-minute progress note?
- Test name and score capture — does it recognize MMPI-3, WAIS-5, WISC-V, Rorschach R-PAS, RBANS, D-KEFS, BRIEF-2, ADOS-2, and capture standardized scores (T-scores, scaled scores, percentile ranks, confidence intervals) into structured fields?
- DSM-5-TR diagnostic specificity — does it produce diagnoses at code-level specificity (F84.0 ASD without language/intellectual impairment; F84.0 with intellectual impairment; F90.2 ADHD combined; F70-F73 Intellectual Developmental Disorder severity levels) including specifiers?
- Forensic and disability evaluation support — does it support the structured format of competency evaluations, disability determinations (SSDI/SSI), Section 504 / IDEA evaluations, and fitness-for-duty assessments?
All products were evaluated in February-April 2026. Pricing and competitor feature claims reflect publicly documented features as of February-April 2026. Custom-priced products were assessed based on disclosed ranges and verified practitioner reports.
Disclosure & methodology. This comparison is published by DeepCura, which is included in the ranking. Pricing and feature claims for competitor products reflect publicly available information as of the evaluation period above and may change — verify directly with each vendor before procurement. This article is editorial commentary; it is not medical, legal, billing, or compliance advice. CPT® is a registered trademark of the American Medical Association. WAIS, WISC, MMPI, Rorschach, ADOS, BASC, Conners, BRIEF, Vineland, and other psychological-test names referenced are trademarks of their respective publishers (Pearson, Hogrefe, MHS, PAR, WPS, Achenbach ASEBA, etc.); DeepCura is not affiliated with, endorsed by, or licensed by any test publisher. References are nominative and used for descriptive comparison only.
Why Psychologists Need an AI Scribe
The Documentation Reality in Clinical Psychology
The clinical psychologist's documentation profile is the most heterogeneous in behavioral health. A typical week in an independent practice includes 50-minute psychotherapy sessions billed under 90834/90837, biopsychosocial intakes under 90791, psychological testing administration under 96136/96137, psychological testing evaluation under 96130/96131, neurobehavioral status exams under 96116/96121, and — depending on the practice — ADHD evaluations, autism spectrum evaluations, learning disability evaluations, dementia evaluations, presurgical psychological evaluations, fitness-for-duty assessments, custody and parenting evaluations, IDEA/504 educational evaluations, disability determinations (SSDI/SSI consultative exams), and competency-to-stand-trial evaluations.
Each documentation product has different conventions, audiences, and audit standards. A 90837 progress note is a brief BIRP/DAP entry of a few hundred words. A psychoeducational evaluation runs 15-30 single-spaced pages with a referral question, comprehensive background, behavioral observations, test-by-test results with confidence intervals, integrated case formulation, DSM-5-TR diagnoses with specifiers, and individualized recommendations addressed to a school IEP team. A forensic report runs even longer, with explicit reference to the legal standard (Dusky standard for competency, MacCAT-CA scores, malingering screening with TOMM/SIRS-2/MFAST), and is read by a judge, opposing counsel, and the court-appointed psychologist or psychiatrist for the other side.
The result is a documentation workload that compounds across formats. Solo and small-group psychology practices regularly report Sunday afternoons spent on report writing because mid-week clinical hours are fully booked, and report turnaround is the most-cited friction in client and referral-source satisfaction. School psychologists, neuropsychologists, and forensic psychologists report the highest weekly documentation hours of any behavioral health profession.
What General-Purpose AI Scribes Miss in Clinical Psychology
Most AI medical scribes are built for a 15-minute medical visit or a 50-minute therapy session. Psychology documentation is fundamentally different in ways that break general-purpose and even therapy-native scribes:
- Long-form integrated report architecture. A psychological evaluation is not a series of progress notes — it is a structured, multi-source document where data from cognitive testing, personality assessment, behavioral observation, collateral interviews, and record review must be integrated into a coherent formulation. The integration step is the clinical value-add, and general-purpose scribes have no concept of report architecture beyond SOAP/BIRP.
- Test-specific score capture. Cognitive batteries (WAIS-5, WISC-V, Stanford-Binet 5, KABC-II) produce standardized scores with confidence intervals — Full Scale IQ, index scores (Verbal Comprehension, Visual Spatial, Fluid Reasoning, Working Memory, Processing Speed in WAIS-5), subtest scaled scores, and percentile ranks. Personality measures (MMPI-3, PAI, MCMI-IV) produce scale-by-scale T-scores with elevation thresholds and validity scale interpretation. Achievement tests (WIAT-4, WJ-IV ACH) produce broad reading, math, and written language composites. The AI must capture these in structured fields, not flatten them into prose.
- Symptom validity and effort testing. Forensic, disability, and many neuropsychological evaluations require formal symptom validity testing — TOMM (Test of Memory Malingering), MFAST (Miller Forensic Assessment of Symptoms Test), SIRS-2 (Structured Interview of Reported Symptoms), Reliable Digit Span, Word Memory Test. The presence and results of effort testing are often dispositive in disability and forensic determinations and must be documented in a defensible structured format.
- Behavioral observations during testing. Standardized testing requires documented behavioral observations — attention, persistence, frustration tolerance, response style, cooperation, rapport, fatigue, special accommodations used. These observations are part of the validity interpretation and are scrutinized in audits and depositions.
- Differential diagnosis and DSM-5-TR specifiers. Psychology evaluations frequently determine specific differential diagnoses with specifiers — F84.0 Autism Spectrum Disorder severity (Level 1, 2, 3), with or without accompanying intellectual impairment, with or without language impairment; F90.2 ADHD severity and predominantly inattentive vs. hyperactive-impulsive vs. combined; F70-F73 Intellectual Developmental Disorder mild/moderate/severe/profound; F81.0 Specific Learning Disorder with impairment in reading (with specifier for word reading accuracy, reading rate/fluency, reading comprehension); F32.0/F32.1/F32.2 MDD severity. A scribe that produces "ASD" or "ADHD" without specifiers fails the documentation standard for educational eligibility, disability determination, and treatment planning.
- Recommendations addressed to specific audiences. Recommendations in a psychoeducational evaluation are addressed to a school team and must align with IDEA-eligible categories and Section 504 frameworks. Recommendations in a forensic evaluation address the court's specific question. Recommendations in a clinical evaluation address the referring provider and the patient. The audience and structure differ markedly.
- Dictation and post-testing report writing. Many psychologists do not record the testing session itself — instead they dictate or write the integrated report after-the-fact based on testing protocol, scoring summaries, behavioral observation notes, and collateral information. The AI workflow needed is post-hoc structured input + integrated report generation, not ambient capture during a 50-minute hour.
Audit, Forensic, and Educational Stakes
Psychological evaluations are audited differently from therapy progress notes. Insurance audits of testing claims (96130-96139) focus on medical necessity, time documentation, integrated interpretation, and the differential consideration of competing diagnoses. School districts review IDEA evaluations for eligibility-determination defensibility. Forensic reports are deposed and cross-examined in court — every opinion must be tied to a data source, and every data source must be documented in admissible format.
State psychology licensing boards investigate documentation in nearly every complaint, and the board orders most frequently cite "inadequate report" or "report does not support diagnostic conclusion" findings. Disability adjudicators (SSDI consultative exam reviewers, ALJs at SSA hearings) read consultative exam reports critically and reject claims supported by reports lacking structured score documentation, behavioral observation, or symptom validity testing where indicated. An AI scribe that captures testing data in structured form, generates DSM-5-TR-aligned diagnoses with specifiers, and produces audience-appropriate recommendations directly reduces deficiencies cited across audit, school, and forensic contexts.
Quick Comparison — Top AI Scribes for Psychologists
| Rank | Tool | Price | Psychology-Specific | EHR Integration | Best For |
|---|---|---|---|---|---|
| 1 | DeepCura | $129/mo | Custom long-form report templates + CDS | 9 EHRs (custom mapping) | Best Overall |
| 2 | Blueprint | ~$59-$99/mo | Measurement-based care | SimplePractice, TherapyNotes | MBC-focused practice |
| 3 | Upheal | ~$59-$99/mo | Telehealth-focused | Limited write-back | Telehealth-only practice |
| 4 | Heidi Health | $0-$99/mo | Generic mental health templates | Limited write-back | Free tier testing |
| 5 | Freed AI | $39-$104/mo | Generic medical, no psych templates | Browser-based EHR push | Solo psychologists adapting general tool |
For a broader cross-specialty comparison, see our Best AI Medical Scribes in 2026 ranking. For therapy-specific tool selection (less testing-focused), see our best AI scribe for therapists guide.
What to Look For in a Psychologist AI Scribe
Psychology documentation is not therapy documentation, and it is not medical documentation. Before choosing a tool, evaluate it against these eight criteria:
1. Long-Form Integrated Report Templates. The AI must support the structured psychological evaluation report architecture: Referral Question and Reason for Evaluation, Sources of Information (records reviewed, collateral interviews, tests administered, time spent), Background Information (presenting concerns, developmental history, medical history, psychiatric history, educational history, occupational/military history, legal history, substance use history, family history, social history), Behavioral Observations During Testing, Test Results by Domain (Cognitive, Academic Achievement, Attention/Executive Function, Memory, Personality/Emotional Functioning, Behavioral Rating Scales, Adaptive Functioning), Integrated Case Formulation, DSM-5-TR Diagnoses with Specifiers, and Recommendations.
2. Standardized Test Score Capture. The AI should recognize and structure scores from major batteries: WAIS-5 (FSIQ, VCI, VSI, FRI, WMI, PSI plus subtests), WISC-V (FSIQ, VCI, VSI, FRI, WMI, PSI), Stanford-Binet 5, KABC-II, MMPI-3 (Validity scales L, K, F, F-r, F-p, F-s; RC scales; Higher-Order scales; Specific Problems scales), PAI (Validity, Clinical, Treatment, Interpersonal scales), Rorschach R-PAS (Engagement and Cognitive Processing, Perception and Thinking Problems, Stress and Distress, Self and Other Representation), RBANS (Immediate Memory, Visuospatial, Language, Attention, Delayed Memory), D-KEFS (Trail Making, Verbal Fluency, Design Fluency, Color-Word Interference, Sorting, 20 Questions, Word Context, Tower, Proverb), WIAT-4 (Reading, Math, Written Expression, Oral Language composites), and behavioral rating scales (BASC-3, CBCL, Conners-4, BRIEF-2, ASRS, Vineland-3).
3. Symptom Validity and Effort Documentation. Forensic, disability, and many neuropsychological reports must document symptom validity and performance validity testing — TOMM with cutoff (≤45 on Trial 2), MFAST results, SIRS-2 if administered, Reliable Digit Span, Word Memory Test, embedded validity indicators on cognitive measures. The AI should capture these in structured fields.
4. DSM-5-TR Diagnostic Specificity with Specifiers. Diagnoses must be at code-level specificity with all DSM-5-TR specifiers: F84.0 ASD with severity (Level 1/2/3) and accompanying impairment specifiers; F90.0/F90.1/F90.2 ADHD with severity (mild/moderate/severe) and presentation; F70-F73 IDD severity; F81.0/F81.1/F81.2 SLD with reading/math/written-expression impairment specifiers; F32.x/F33.x MDD with episode/recurrence/severity/specifiers (severity-graded specifiers including mood-quality and onset modifiers per DSM-5-TR); F43.81 Prolonged Grief Disorder; F60.3 Borderline Personality Disorder.
5. Recommendations Architecture. Recommendations in a psychoeducational evaluation must align with IDEA categories (Specific Learning Disability, Other Health Impairment, Autism, Emotional Disturbance, Intellectual Disability, Speech-Language Impairment, etc.) or Section 504 frameworks. Recommendations in a forensic report must address the court's question. Recommendations in a clinical evaluation address the referring provider and patient. The AI should support audience-specific recommendation generation.
6. CPT 96xxx Testing Code Capture. Time documentation for 96130 (psychological testing evaluation, first hour), 96131 (each additional hour), 96132 (neuropsych eval, first hour), 96133 (each additional hour), 96136/96137 (psychological testing administration, technician or psychologist), 96138/96139 (neuropsych testing administration), 96116/96121 (neurobehavioral status exam), 96146 (computerized testing). Audit-defensible time documentation is essential since payers scrutinize testing units more than therapy units.
7. Behavioral Rating Scale Aggregation. Pediatric and ADHD evaluations rely heavily on multi-rater behavioral assessment — BASC-3 (parent, teacher, self-report), Conners-4 (parent, teacher, self-report), BRIEF-2 (parent, teacher, self-report), CBCL/TRF/YSR (Achenbach system). The AI should support multi-rater data aggregation and cross-informant analysis (e.g., "Parent and teacher both rated Hyperactivity-Impulsivity in the Clinically Significant range; self-report was within normal limits — consistent with informant-context discordance commonly seen in adolescents").
8. EHR Integration with Therapy and Testing-Capable Platforms. SimplePractice, TherapyNotes, TheraNest, and ICANotes are dominant in clinical psychology private practice. Some psychologists use specialty platforms (Q-interactive for digital test administration, Q-global for scoring, WPS Online Evaluation System for selected measures). Bidirectional integration with the practice management EHR is the highest-leverage friction reduction for the long-form report workflow.
Detailed Reviews
1. DeepCura — Best Overall for Clinical Psychology Practice
DeepCura is a customizable clinical AI platform that combines ambient scribing, clinical decision support, evidence search, practice automation, and bidirectional EHR integration — $129/month with unlimited notes. For clinical psychologists in independent practice — particularly those running mixed therapy-and-testing caseloads, neuropsychologists, child and adolescent psychologists, and forensic psychologists — DeepCura's customizable templates deliver a strong fit because no off-the-shelf therapy-AI tool supports the long-form integrated report architecture.
For psychologists, the key differentiator is template depth. DeepCura's custom template builder lets clinicians encode multi-section integrated report templates: a psychoeducational evaluation template with sections for Referral Question, Background, Behavioral Observations, Cognitive Testing (with WISC-V subtest score fields), Achievement Testing (with WIAT-4 composite fields), Behavior Rating Scales (with BASC-3 multi-rater fields), Integrated Formulation, DSM-5-TR Diagnoses with Specifiers, and IDEA-aligned Recommendations. A neuropsychological evaluation template encodes different fields — Cognitive Domains (Attention, Memory, Executive Function, Language, Visuospatial, Processing Speed), Symptom Validity (TOMM/MFAST), Effort, and Functional Implications. A forensic report template encodes the legal question, MacCAT-CA, malingering screening, Dusky-standard analysis, and conclusions addressed to the court.
CDS Mode (3 credits per evaluation) generates differential diagnostic considerations during testing interpretation — useful for ambiguous presentations like the adolescent who presents with attention difficulties, mood lability, learning struggles, and social difficulties where the differential may include ADHD, MDD, ASD without intellectual impairment, SLD, or post-traumatic responses. The differential is part of the integrated formulation and supports the documented clinical reasoning that auditors and IEP teams require.
DeepEvidentia — DeepCura's evidence search engine — pulls from PubMed, APA Division 12 evidence-based practice resources, NAN (National Academy of Neuropsychology) position papers, AAMR (American Association on Mental Retardation, now AAIDD), and IDEA regulatory resources. "WISC-V FSIQ vs GAI when discrepancy is present" returns Watkins et al. and the WISC-V Technical Manual recommendation. "TOMM cutoff in litigation cases" surfaces Tombaugh's manual and replication studies. "ADOS-2 vs ADI-R diagnostic accuracy in school-age children" returns Falkmer et al. systematic review.
Strengths:
- Custom template builder for multi-section integrated reports (psychoeducational, neuropsychological, ADHD, ASD, forensic, disability)
- CDS Mode with differential diagnostic considerations during interpretation (3 credits per evaluation)
- DeepEvidentia evidence search (PubMed, APA Div 12, NAN, AAIDD, IDEA regulatory access)
- AI receptionist for after-hours intake and referral routing — particularly valuable for testing-heavy practices that take referrals from schools, attorneys, and physicians
- Multiple AI engines matched to encounter complexity (1-15 credits)
- Custom templates for therapy progress notes (BIRP/DAP) coexist with long-form report templates — one platform handles both ends of the practice
- Treatment plan generator with SMART goals for therapy clients
- Bidirectional integration with major EHRs and SimplePractice/TherapyNotes via custom field mapping
- Unlimited notes on all plans — important for psychologists who produce 4-6 reports plus 20+ progress notes weekly
Limitations:
- Custom template builder requires meaningful initial setup (8-15 hours for a psychologist running 4-6 distinct evaluation types to encode templates with score-field structures)
- Standardized test score interpretation is not pre-loaded — psychologists encode score thresholds and interpretive logic into their templates rather than receiving them out of the box
- CDS Mode trained on broad medical literature — psychology-specific differentials and test-interpretation nuances require validation by the clinician
Pricing: $129/month per provider — all features included. Free trial available, no credit card required.
Verdict: DeepCura is the strongest choice for psychology practices that need a platform supporting both therapy progress notes AND long-form integrated reports — which is most independent psychology practices. The flexibility cost is upfront setup time, but for psychologists who currently spend 20+ hours per week on report writing, the per-report time savings compound quickly. Testing-and-therapy psychologists benefit most from DeepCura's depth.
DeepCura: Customizable AI Scribe for Clinical Psychology
Custom long-form integrated report templates, BIRP/DAP for therapy notes, AI receptionist for after-hours intake, evidence search, and unlimited reports — $129/mo. Start your free trial.
+1 (415) 549-1829Available 24/7 · Set up in seconds · No credit card required
2. Blueprint — Best for Measurement-Based Psychology
Blueprint is a behavioral health measurement-based care platform that has expanded into AI-assisted documentation. The original product centers on automated administration of validated measures (PHQ-9, GAD-7, PCL-5, OQ-45, ACE, C-SSRS, BASC-3 short forms, ORS/SRS) to clients before sessions, with results flowing into the chart and trending over time. The AI scribe addition generates progress notes that explicitly cite measurement results and document treatment response as a function of measure trajectory.
For psychologists who run outcome-focused practices — particularly those who use the Patient-Focused Outcomes Research methodology, who contract with payers requiring measurement-based care, or who want measure-trended documentation in published research — Blueprint's measurement infrastructure is the most targeted of the tools reviewed. Some psychologists also use Blueprint's measurement library as a screening front-end for testing referrals.
The limitation for psychologists is that Blueprint does not produce long-form integrated reports. The AI scribe component covers measure-aware progress notes, not multi-section evaluation reports.
Pricing: Approximately $59-$99/month per clinician depending on plan and measure library access.
Verdict: Best for therapy-focused psychology practices invested in measurement-based care, particularly those contracted with payer networks requiring it. Not a fit for psychologists whose primary documentation product is the long-form psychological or neuropsychological evaluation report.
3. Upheal — Best for Telehealth-Only Psychology Practices
Upheal targets the telehealth-only behavioral health segment with native integration into the video-session workflow. Session is recorded and transcribed within Upheal's video platform; the AI generates the progress note in BIRP, DAP, or SOAP format; the clinician reviews and signs. For psychologists running fully telehealth therapy practices, Upheal's integrated video-and-documentation workflow eliminates the friction of using separate platforms.
The limitations for psychologists are scope and report depth. Upheal works best as a telehealth-native therapy tool — psychologists who do in-person testing or in-person therapy need a separate solution for those encounters, and Upheal's modality and report-template depth is narrower than DeepCura's. Long-form integrated reports are not in scope.
Pricing: Approximately $59-$99/month per clinician depending on tier.
Verdict: Best for psychologists running fully telehealth therapy practices who want one integrated video-and-documentation platform. Not a fit for testing-heavy practices or mixed in-person/telehealth practices.
4. Heidi Health — Best Free Tier for Solo Psychologists
Heidi Health offers a usable free tier (limited notes per month) before paid plans kick in at the Pro level — the only credible no-cost entry point for solo psychologists testing AI documentation. Heidi was originally human-medicine focused but has added BIRP, DAP, and SOAP therapy templates as part of its specialty expansion.
Heidi has stronger product traction in Australia, New Zealand, and the UK than in North America, and its mental health templates reflect international payer and DSM/ICD conventions more than US-specific testing-evaluation conventions. Long-form integrated reports are not currently in Heidi's template library, and PIMS integration is limited (clipboard or email rather than direct API write-back).
Pricing: Free tier (limited notes), Pro tier roughly $129/month, enterprise tier higher.
Verdict: Best for solo psychologists who want to test ambient AI documentation at zero cost on therapy progress notes before committing to a paid tool. Not a fit for testing-evaluation workflows. For an in-depth review, read our Heidi Health review.
5. Freed AI — Simplest Ambient Without Psychology Templates
Freed AI is a clean, fast ambient scribe for primary care medicine with a tiered Free-to-Premier pricing structure. Solo psychologists sometimes adopt Freed because the price is accessible ($39-$104/month) and the ambient experience is good, but Freed has no psychology-specific templates — no BIRP/DAP, no DSM-5-TR-aware diagnostic structure, no integrated report architecture, no testing score fields, and no measurement-based-care fields.
Practical effect: Freed transcribes the session, generates a generic SOAP note structured for medical documentation, and the psychologist reformats into the format expected by their EHR and payer. The time savings for therapy progress notes are smaller than with a therapy-native tool, and any testing or evaluation work requires complete manual reformatting.
Pricing: $39/month (Starter, 40 notes), $79/month (Core, unlimited), $104/month (Premier, unlimited + EHR push + ICD-10).
Verdict: Adequate as a stopgap for solo psychologists testing the ambient AI category before committing to a therapy-native or therapy-customizable tool. Not recommended as a long-term primary scribe for psychology practice. Read our Freed AI review.
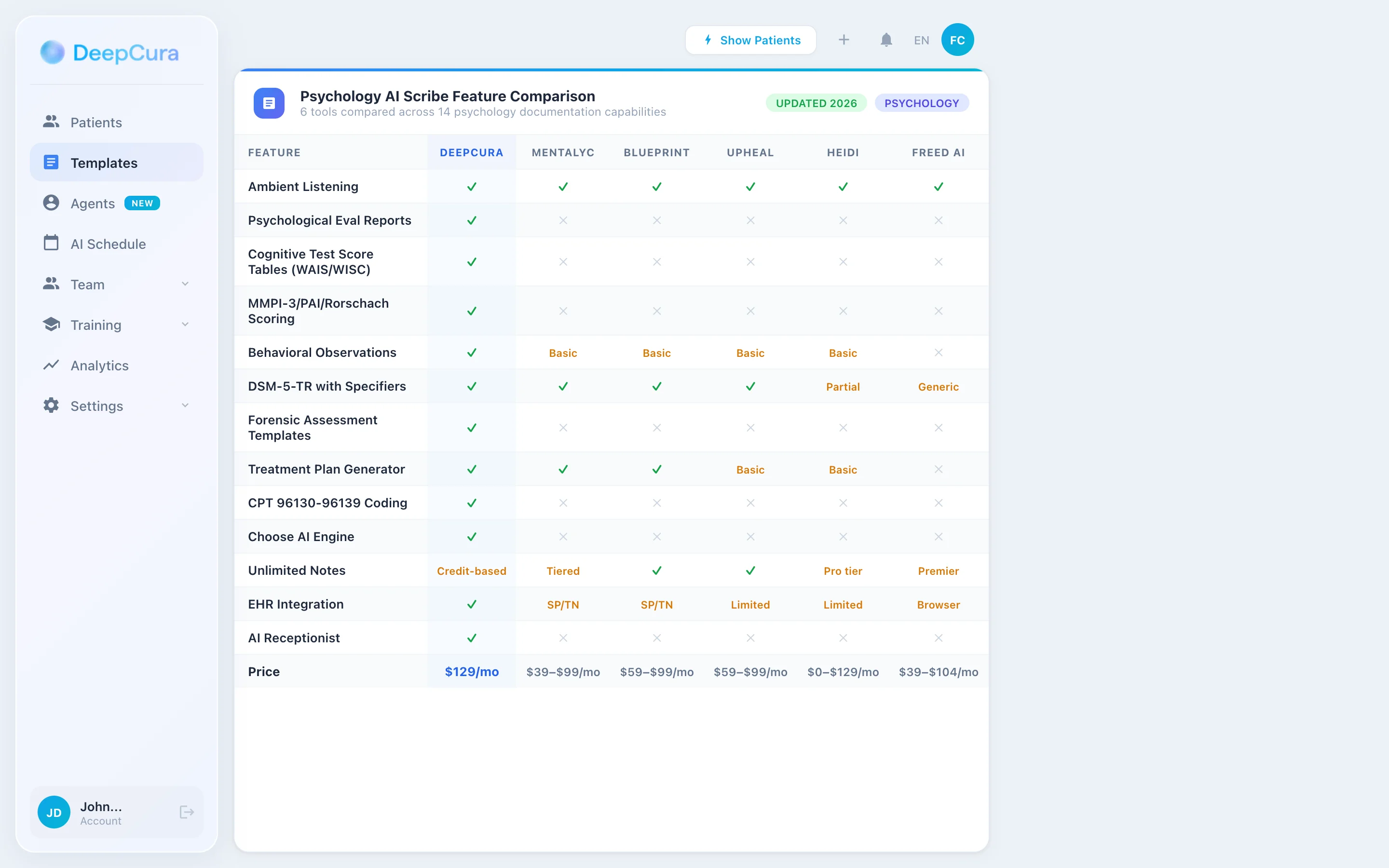
Head-to-Head — Psychology Documentation Features
| Feature | DeepCura | Blueprint | Upheal | Heidi | Freed |
|---|---|---|---|---|---|
| Therapy Progress Notes (BIRP/DAP) | Custom | ✓ | ✓ | Partial | ✗ |
| Long-Form Integrated Reports | ✓ Custom | ✗ | ✗ | ✗ | ✗ |
| Psychoeducational Evaluation Template | ✓ Custom | ✗ | ✗ | ✗ | ✗ |
| Neuropsych Evaluation Template | ✓ Custom | ✗ | ✗ | ✗ | ✗ |
| ADHD/ASD Evaluation Template | ✓ Custom | ✗ | ✗ | ✗ | ✗ |
| Forensic / Disability Eval Template | ✓ Custom | ✗ | ✗ | ✗ | ✗ |
| User-Entered Score Fields | ✓ Configurable templates | ✗ | ✗ | ✗ | ✗ |
| Symptom Validity (TOMM/MFAST/SIRS-2) | ✓ Custom | ✗ | ✗ | ✗ | ✗ |
| DSM-5-TR Code-Level + Specifiers | ✓ | ✓ | ✓ | Partial | Generic |
| Risk Assessment (C-SSRS, SI/HI) | ✓ structured | ✓ structured | Partial | Partial | ✗ |
| Measurement-Based Care | ✓ | ✓ (core focus) | Partial | Partial | ✗ |
| CPT 96130-96139 Testing Code Capture | ✓ | ✗ | ✗ | ✗ | ✗ |
| Clinical Decision Support | ✓ (differentials) | ✗ | ✗ | ✗ | ✗ |
| EHR Bidirectional | Custom mapping | SimplePractice/TherapyNotes | Limited | Limited | Browser-based EHR push |
| Price | $129/mo | ~$59-$99/mo | ~$59-$99/mo | $0-$99/mo | $39-$104/mo |
Psychology Documentation Workflow with DeepCura
DeepCura's tiered credit system lets psychologists match AI resources to documentation complexity — fast for therapy progress notes, deeper for full integrated evaluations.
Therapy Progress Note (1 Credit) — 90834 / 90837 Individual Sessions
For routine 45-minute or 53+ minute individual psychotherapy sessions within an established treatment plan — CBT for MDD, DBT skill review, EMDR Phase 4-7 processing, IFS unburdening — the 1-credit model generates a BIRP or DAP note in under 30 seconds with intervention, response, treatment plan goal alignment, and next-session plan. Speed-optimized for the high-volume clinical day where a psychologist runs 6-8 individual sessions back-to-back.
Biopsychosocial Intake (3 Credits CDS) — 90791 Diagnostic Evaluation
For new client diagnostic evaluations — comprehensive history, MSE, risk assessment, ACE screen, working diagnostic formulation, and treatment plan draft — CDS Mode activates differential diagnostic generation. The AI structures the biopsychosocial across the standard sections and surfaces differential considerations: in a client presenting with chronic interpersonal instability, affect dysregulation, and self-harm history, the differential includes Borderline Personality Disorder, Complex PTSD, Bipolar II, and ADHD with rejection sensitivity — each of which has different first-line treatment recommendations.
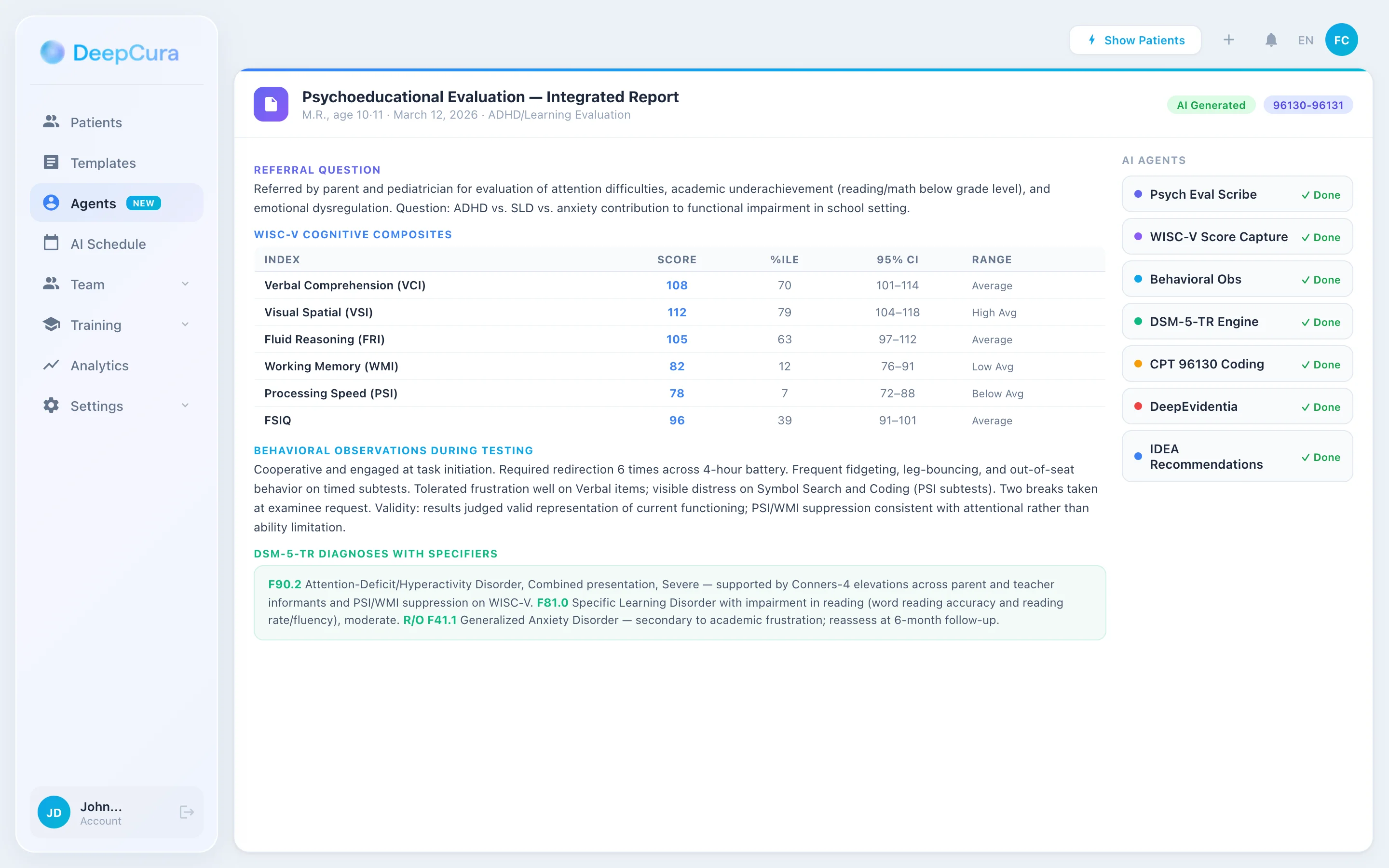
Long-Form Integrated Report (15 Credits) — 96130-96133 Psychological Testing Evaluation
For psychoeducational evaluations, neuropsychological evaluations, ADHD evaluations, ASD evaluations, forensic reports, and disability determinations — the maximum-depth model produces complete multi-section integrated reports. The psychologist provides the testing protocol (raw scores, scaled scores, T-scores, percentile ranks, behavioral observations, collateral information, records reviewed) into structured input fields; the AI generates the integrated report sections (background, observations, results-by-domain, formulation, diagnoses with specifiers, recommendations) in a coherent narrative that integrates across data sources rather than producing disconnected score listings.
From Score Sheet to Integrated Report in Minutes
DeepCura's 15-credit long-form report engine takes raw scores, behavioral observations, and collateral data and produces an integrated multi-section evaluation report with DSM-5-TR diagnoses and audience-aligned recommendations. Start your free trial.
+1 (415) 549-1829Available 24/7 · Set up in seconds · No credit card required
Clinical Decision Support and Evidence Search for Psychologists
CDS Mode — Differentials and Diagnostic Refinement
CDS Mode outputs are documentation-aid suggestions for clinician review. They are not diagnoses, treatment recommendations, or substitutes for clinical judgment. The psychologist retains full responsibility for diagnostic conclusions, test interpretation, and treatment recommendations. DeepCura is not an FDA-cleared medical device.
Psychology evaluation is differential diagnosis at high resolution. The 12-year-old presenting with attention difficulties, learning struggles, and social differences could be ASD without intellectual impairment, ADHD-Combined Type, SLD with reading impairment, post-traumatic responses, generalized anxiety, or some combination. The 45-year-old presenting with cognitive complaints could be early-onset Alzheimer's, vascular cognitive impairment, depression-related cognitive impairment ("pseudodementia"), TBI sequelae, anxiety-driven cognitive load, or symptom magnification in a litigation context. CDS Mode generates differential considerations alongside the report — flagging high-yield rule-outs and ruling-in considerations that affect the integrated formulation.
For a 16-year-old presenting with mood symptoms, sleep dysregulation, family conflict, and recent academic decline, CDS Mode flags: MDD recurrent, Bipolar II Depression with mixed features, Adjustment Disorder, Substance/Medication-Induced Mood Disorder, Disruptive Mood Dysregulation Disorder (rule-out given age), and family-system stressors. The differential becomes part of the integrated formulation and the documented clinical reasoning.
No competitor in this comparison integrates clinical decision support into the documentation workflow. Blueprint, Upheal, Heidi, and Freed are documentation-only tools. DeepCura adds the clinical reasoning layer that supports both interpretation and the documented reasoning in the report.
DeepEvidentia — Evidence at the Bedside for Psychologists
DeepEvidentia provides real-time access to PubMed, APA Division 12 evidence-based practice resources, NAN position papers, AAIDD documentation, IDEA regulatory resources, Cochrane reviews, and treatment-manual references directly within the documentation workflow.
Example queries psychologists actually ask:
- "WISC-V GAI vs FSIQ when index discrepancy is present" — returns Watkins et al. and the WISC-V Technical Manual recommendation
- "TOMM cutoff in litigation cases" — surfaces Tombaugh's manual, Greve et al. base rate studies, and replication research
- "ADOS-2 vs ADI-R diagnostic accuracy in school-age children" — returns Falkmer et al. systematic review and Risi et al.
- "MMPI-3 RC scale interpretation in dual-diagnosis pain populations" — surfaces Ben-Porath et al. RC scale validity studies
- "Reliable change index for WAIS-5 retest in TBI assessment" — returns the WAIS-5 reliable change tables and Iverson critique
- "Stanley-Brown Safety Planning Intervention validated outcomes" — returns the original Stanley & Brown 2012 paper and replication
For complex case formulation, peer consultation prep, and informed-consent discussions about diagnosis and treatment recommendations, evidence access at the bedside transforms documentation time into clinical reasoning time.
Pricing Comparison
| Tool | Monthly | Note Limit | Long-Form Reports | Best Plan |
|---|---|---|---|---|
| DeepCura | $129/mo | Unlimited | ✓ (15 credits/report) | Single plan, all features |
| Blueprint | ~$59-$99/mo | Unlimited | ✗ | MBC + AI scribe combined |
| Upheal | ~$59-$99/mo | Unlimited | ✗ | Standard with telehealth integration |
| Heidi Health | $0-$99/mo | Free tier limited | ✗ | Free or Pro |
| Freed AI | $39-$104/mo | 40-unlimited | ✗ | Core ($79) or Premier ($104) |
See DeepCura in Action
Watch how DeepCura handles the full clinical workflow — ambient progress note generation, biopsychosocial intake with differential generation, long-form integrated report generation with score capture and DSM-5-TR-specifier diagnoses, evidence search, and AI receptionist for after-hours intake.

Frequently Asked Questions
What is the best AI scribe for psychologists?
DeepCura is the strongest cross-functional choice for psychology practices that produce both therapy progress notes AND long-form psychological evaluation reports — which is most independent psychology practices. For psychologists whose practice is primarily psychotherapy with measurement-based care contracts, Blueprint is a strong purpose-built alternative. For fully telehealth therapy practices, Upheal's integrated video-and-documentation workflow is the path of least resistance — though only DeepCura supports long-form integrated reports.
Do AI scribes generate psychological evaluation reports with WAIS, MMPI, and Rorschach scores?
DeepCura supports custom long-form integrated report templates with user-configurable fields where the psychologist enters scores from any battery they have administered. DeepCura does not administer, score, or interpret psychological tests — score interpretation remains the psychologist's responsibility. No therapy-native AI scribe (Blueprint, Upheal) supports long-form integrated reports out of the box. The AI structures the data and integrates the narrative, but standardized score thresholds and interpretive logic must be encoded into the template by the practitioner during setup.
Can AI scribes document forensic and disability evaluations defensibly?
DeepCura's customizable templates can be configured for forensic competency-to-stand-trial evaluations (with MacCAT-CA structure, Dusky-standard analysis, malingering screening with TOMM/SIRS-2/MFAST), disability evaluations (SSDI/SSI consultative exam structure with symptom validity and effort documentation), and IDEA/Section 504 educational evaluations. The AI structures the report; the psychologist remains responsible for defensible opinions and conclusions, deposition-readiness of every cited data source, and chain-of-custody for testing protocols.
Do AI scribes integrate with SimplePractice, TherapyNotes, and Q-global / Q-interactive?
Therapy practice management EHRs (SimplePractice, TherapyNotes) integrate with Blueprint and DeepCura via field-mapping. Q-global (Pearson scoring), Q-interactive (Pearson digital test administration), and WPS Online Evaluation System are testing-specific platforms that operate alongside but separately from the AI scribe — psychologists score in Q-global and bring scores into the AI report template manually or via export-paste. No AI scribe currently has direct API integration with Pearson Q-global or WPS, though DeepCura's structured score-capture fields make the manual entry workflow more efficient than narrative-only tools.
Are AI scribes compliant with HIPAA, FERPA (school evaluations), and 42 CFR Part 2?
Reputable AI scribes operate under HIPAA Business Associate Agreements with encryption in transit and at rest. School evaluations conducted under IDEA/504 are typically governed by FERPA when records are maintained in the student's educational file — psychologists conducting school-based or IEP-related evaluations should confirm with the school district whether the vendor's data-handling agreement satisfies the district's FERPA-aligned requirements, which sometimes exceed HIPAA. 42 CFR Part 2 (substance use disorder records) imposes additional consent and disclosure requirements beyond HIPAA. DeepCura signs HIPAA BAAs. Customers handling 42 CFR Part 2 records remain responsible for Part 2 consent and redisclosure controls. Verify each vendor's Part 2 posture independently.
Can AI scribes capture C-SSRS, PHQ-9, GAD-7, and behavior rating scales like BASC-3?
Therapy-native tools and customizable platforms support measurement-based care capture. Blueprint is the most measurement-focused platform — administering measures pre-session and surfacing trends. DeepCura captures measure scores from the session conversation or from manual structured-field entry; multi-rater behavior rating scales (BASC-3 parent/teacher/self-report; Conners-4 parent/teacher/self-report; BRIEF-2 parent/teacher/self-report) are encoded in templates as multi-rater fields with cross-informant aggregation prompts.
How much do AI scribes for psychologists cost?
Pricing ranges from a free Heidi tier through enterprise. Blueprint and Upheal are in the $59-$99/month range. Freed starts at $39/month. DeepCura is $129/month with unlimited notes, CDS, evidence search, AI receptionist, and customizable templates including long-form integrated reports. For most independent psychology practices producing 4-6 evaluation reports per month plus 20+ therapy notes weekly, DeepCura's per-report time savings on integrated evaluations alone typically justify the price differential vs therapy-only alternatives.
Do clients object to ambient AI recording during testing or therapy sessions?
Most psychologists do not record the testing administration itself — testing is an in-vivo standardized procedure where the psychologist captures responses, behavioral observations, and timing during administration, and the AI workflow involves post-administration structured input rather than ambient capture. For therapy sessions, clients are more likely to raise concerns than medical patients because the therapeutic frame is the treatment. Discuss AI documentation in informed consent at intake, document client consent (or refusal) in the chart, and offer an opt-out workflow for clients who decline.
Final Verdict
For psychologists in independent practice, the choice comes down to three profiles:
Best overall: DeepCura at $129/month — customizable long-form integrated report templates (psychoeducational, neuropsychological, ADHD, ASD, forensic, disability), BIRP/DAP for therapy progress notes, CDS differentials, evidence search via DeepEvidentia, AI receptionist for after-hours intake routing, and unlimited notes. The strongest choice for psychologists whose practice includes both therapy and testing — which is most independent clinical psychology practice — and the only platform reviewed that supports long-form integrated report generation.
Best for measurement-based practice: Blueprint at $59-$99/month — measurement-based care platform with AI scribe integrated. Best for psychology practices contracted with payer networks requiring measurement-based care or running outcome-focused supervision and quality assurance.
Best for telehealth-only therapy: Upheal at $59-$99/month — integrated video-and-documentation platform with BIRP, DAP, and SOAP support. The path of least resistance for psychologists running fully telehealth psychotherapy practices, though long-form integrated reports are not in scope.
For a broader cross-specialty comparison, see our Best AI Medical Scribes in 2026 ranking. For therapy-specific tool selection (less testing-focused), see our best AI scribe for therapists guide. For psychiatrists managing medication, see our best AI scribe for psychiatry ranking. For free copy-paste clinical templates, see our SOAP note template and biopsychosocial assessment references. For practices needing after-hours crisis screening alongside documentation, see our Best AI Medical Receptionist guide. For EMR evaluation alongside the scribe decision, see our best EMR for small practices ranking.
References
[1] American Psychological Association, "2024 APA Workforce Analysis," APA. apa.org/workforce
[2] American Psychiatric Association, "Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR)," APA Publishing, 2022. psychiatry.org/dsm5
[3] Greve KW, Bianchini KJ, "Setting empirical cut-offs on psychometric indicators of negative response bias: A methodological commentary with recommendations," Archives of Clinical Neuropsychology, 19(4), 533-541, 2004. pubmed.ncbi.nlm.nih.gov/15163457
[4] Falkmer T, Anderson K, Falkmer M, Horlin C, "Diagnostic procedures in autism spectrum disorders: a systematic literature review," European Child & Adolescent Psychiatry, 22(6), 329-340, 2013. pubmed.ncbi.nlm.nih.gov/23322184
[5] American Educational Research Association, American Psychological Association, National Council on Measurement in Education, "Standards for Educational and Psychological Testing," AERA, 2014. apa.org/science/programs/testing/standards
[6] American Medical Association, "CPT 2026 Professional Edition — Psychological and Neuropsychological Testing CPT Codes (96116, 96121, 96130-96133, 96136-96139, 96146)," AMA. ama-assn.org/practice-management/cpt
[7] U.S. Department of Education, "Individuals with Disabilities Education Act (IDEA) — Sec. 300.304-311 Evaluation Procedures," IDEA. sites.ed.gov/idea
[8] Posner K, Brown GK, Stanley B, et al, "The Columbia–Suicide Severity Rating Scale: Initial Validity and Internal Consistency Findings," American Journal of Psychiatry, 168(12), 2011. cssrs.columbia.edu
[9] American Psychological Association Division 12, "Society of Clinical Psychology — Research-Supported Psychological Treatments," Div 12. div12.org
[10] National Academy of Neuropsychology, "NAN Position Papers on Test Security, Symptom Validity, and Computerized Assessment," NAN. nanonline.org