Registered nurses spend 25-50% of their shift on documentation depending on setting — med-surg RNs charting q4h vitals and assessments, ICU RNs documenting q1-2h hemodynamics and continuous infusion titration, home health RNs producing OASIS-E assessments, school nurses managing daily medication administration logs, and case management RNs writing care coordination narratives — and the documentation tax is the leading cited driver of nurse turnover ahead of compensation, ratios, and scheduling. The 2024 NCSBN nurse workforce study found that nurses cite "time spent on documentation that pulls them away from the bedside" as the single most demoralizing operational factor in their work.
We ranked 6 AI scribes on the criteria that matter most for nursing documentation:
- Nursing process and ADPIE structure — does the AI support NANDA-I nursing diagnoses, ADPIE (Assessment, Diagnosis, Planning, Implementation, Evaluation) workflow, and standardized nursing care plan documentation?
- Risk assessment scale capture — does it capture Braden Scale (pressure injury), Morse Falls Scale, Hendrich II, MEWS / NEWS2 (early warning), CIWA-Ar (alcohol withdrawal), and pain scales (NRS, FLACC, PAINAD, Wong-Baker FACES)?
- SBAR handoff support — does it produce structured SBAR (Situation, Background, Assessment, Recommendation) and ISBAR/IPASS handoff documents at shift change, transfer of care, or rapid response team activation?
- Setting-aware templates — does it produce different note structures for med-surg q4h assessments vs ICU q1-2h hemodynamics vs ED triage vs L&D delivery vs home health OASIS-E vs school nurse daily log?
All products were evaluated in February-April 2026. Pricing reflects publicly available rates. AI scribe adoption among bedside RNs is earlier-stage than among physicians and APPs; integration depth varies meaningfully by hospital system and EHR.
Disclosure & methodology. This comparison is published by DeepCura, which is included in the ranking. Pricing and feature claims for competitor products reflect publicly available information as of the evaluation period above and may change — verify directly with each vendor before procurement. This article is editorial commentary; it is not medical, legal, billing, or compliance advice. CPT® is a registered trademark of the American Medical Association. NANDA-I® is a registered trademark of NANDA International, Inc.; The Joint Commission and I-PASS are registered trademarks of their respective owners. All other product names and trademarks are property of their respective owners; references are nominative and do not imply affiliation or endorsement.
Why Nurses Need an AI Scribe
The Documentation Reality at the Bedside
Nursing documentation occupies a different position in the chart than physician or APP documentation. Where physicians and APPs produce a single comprehensive note per encounter, nurses produce multiple documentation products throughout each shift:
- Initial assessment at start of shift — head-to-toe assessment, baseline vitals, pain, fall risk, pressure injury risk, mental status, code status review, line/tube/drain inventory
- Ongoing assessments at protocol-driven intervals (q4h med-surg, q2h step-down, q1-2h ICU)
- Medication administration records (eMAR) with the 5 rights and structured exception documentation
- Intake and output (I&O) tallies, often hourly in critical care
- Procedure and intervention notes for IV starts, blood draws, foley insertion, NG insertion, dressing changes, central line care, ventilator changes, infusion titration
- Pain reassessment post-intervention per organizational policy
- Education and discharge teaching documentation with teach-back validation
- Care coordination — interdisciplinary rounds, family meetings, social work and case management touchpoints, transfer of care
- Rapid response and code documentation with timeline accuracy required for resuscitation review
- End-of-shift summary and SBAR handoff to oncoming staff
- Incident and variance reporting for falls, medication errors, line failures, equipment issues — separate from clinical chart but legally consequential
The 2024 NCSBN nurse workforce data documented that the average med-surg RN spends 35-40% of clinical time on documentation, ICU RNs 40-50%, and home health RNs 50%+. The administrative load is the most-cited factor in burnout and bedside-to-non-bedside transition decisions across surveys conducted by ANA, NCSBN, AACN, and major hospital systems.
What General-Purpose AI Scribes Miss in Nursing Practice
Most AI medical scribes are built around a 15-minute physician-patient encounter — ambient capture of an HPI, focused exam, MDM, and plan. Nursing documentation is fundamentally different in ways that break general-purpose scribes:
- Continuous assessment, not episodic encounter. Nursing documentation runs the entire shift. The unit of work is not a 15-minute conversation but a 12-hour continuum of patient observation, intervention, and reassessment. Ambient capture during a brief bedside interaction misses the context of the prior 4 hours.
- NANDA-I nursing diagnoses, not ICD-10. Nursing diagnoses (NANDA-I 2024-2026 edition) describe the patient's response to a health condition — Acute Pain (00132), Risk for Falls (00155), Impaired Skin Integrity (00046), Anxiety (00146), Ineffective Airway Clearance (00031), Risk for Infection (00004), Imbalanced Nutrition: Less Than Body Requirements (00002), Deficient Knowledge (00126). These are distinct from ICD-10 medical diagnoses and drive the nursing care plan. A scribe that only knows ICD-10 cannot generate nursing-language diagnoses.
- ADPIE structure. Nursing notes follow ADPIE (Assessment, Diagnosis, Planning, Implementation, Evaluation) or DAR (Data, Action, Response) for focused notes. Some institutions use FDAR (Focus, Data, Action, Response). These are nursing-specific note structures the AI must support — not SOAP or BIRP.
- Risk scale documentation. Braden Scale (pressure injury risk, 6-23 points; ≤18 = at risk), Morse Falls Scale (0-125; ≥45 high risk), Hendrich II Fall Risk Model, NEWS2 (National Early Warning Score 2 for clinical deterioration), MEWS (Modified Early Warning Score), CIWA-Ar (Clinical Institute Withdrawal Assessment for alcohol revised), CINA (Clinical Institute Narcotic Assessment), Glasgow Coma Scale (3-15), RASS (Richmond Agitation-Sedation Scale -5 to +4), CAM (Confusion Assessment Method) for delirium, BPS (Behavioral Pain Scale) for non-verbal patients, CPOT (Critical-Care Pain Observation Tool). These are nurse-administered, nurse-documented, and nurse-trended.
- Pain scales by patient population. NRS 0-10 for verbal adults, Wong-Baker FACES for pediatrics and limited literacy, FLACC (Face, Legs, Activity, Cry, Consolability) for pediatric non-verbal and post-operative, PAINAD (Pain Assessment in Advanced Dementia) for advanced dementia patients, BPS and CPOT for ICU patients on mechanical ventilation. The AI must select the appropriate scale by population.
- SBAR and structured handoff. SBAR (Situation, Background, Assessment, Recommendation) and IPASS (Illness severity, Patient summary, Action list, Situation awareness/contingency planning, Synthesis by receiver) are the structured handoff formats nurses use at shift change, transfer of care, and rapid response activation. The AI should generate these from the shift's documentation rather than requiring separate dictation.
- Five Rights of Medication Administration. Right patient, right drug, right dose, right route, right time — and increasingly Right Documentation, Right Reason, Right Response (the 8 Rights). Medication administration documentation is high-stakes and audited carefully.
- Setting-specific templates. Med-surg q4h documentation differs from ICU q1-2h hemodynamics from ED triage from L&D delivery documentation from home health OASIS-E from hospice IDG (Interdisciplinary Group) documentation from school nurse daily medication log from occupational health post-incident documentation. A single template fails across these settings.
Audit, Quality, and Patient Safety Stakes
Nursing documentation has direct quality and patient-safety consequences. CMS SEP-1 sepsis bundle compliance requires nurse-driven documentation of lactate redraw, antibiotic administration, fluid resuscitation, and vasopressor initiation against time-stamped clocks. CAUTI (Catheter-Associated Urinary Tract Infection), CLABSI (Central Line-Associated Bloodstream Infection), VAP (Ventilator-Associated Pneumonia), and SSI (Surgical Site Infection) prevention bundles are nurse-driven with documentation requirements that affect both quality scores and value-based-purchasing penalties. HCAHPS scores are partly tied to nursing communication and pain management documentation.
The Joint Commission (TJC) audits nursing documentation specifically — pain reassessment after intervention, restraint use documentation, falls assessment and reassessment, blood transfusion documentation, code/RRT timeline accuracy. Variance from policy in the chart is the most common deficiency cited in TJC findings. State Boards of Nursing investigate documentation in nearly every complaint, and the most common finding cited in board orders is "inadequate or untimely nursing documentation."
An AI scribe that supports ADPIE structure, NANDA-I diagnoses, risk scale capture, SBAR handoff, the 5 Rights of medication administration, and setting-specific templates directly affects audit defensibility, quality program performance, and patient safety outcomes.
Quick Comparison — Top AI Scribes for Nurses
| Rank | Tool | Price | Nursing-Specific | EHR Integration | Best For |
|---|---|---|---|---|---|
| 1 | DeepCura | $129/mo | Custom ADPIE + NANDA + risk-scale templates | 9 EHR integrations (Epic, Cerner via HL7/FHIR with custom field mapping; native integrations for athenahealth, AdvancedMD, eClinicalWorks) | Best Overall |
| 2 | Abridge AI | Custom enterprise | Enterprise multi-role nursing | Epic deep | Hospital systems |
| 3 | Nuance DAX Copilot | Custom enterprise | Enterprise EHR-native | Epic, Cerner deep | Epic/Cerner shops |
| 4 | Suki AI | ~$199/mo | Voice-first ambient + dictation | Epic, Cerner, athenahealth | Voice-first nursing |
| 5 | Heidi Health | $0-$99/mo | Generic templates, nursing-adaptable | Limited write-back | Free tier RN trial |
| 6 | Freed AI | $39-$104/mo | NP-friendly, basic for RN | Browser scrape (Premier) | Nurse practitioners |
For a broader cross-specialty comparison, see our Best AI Medical Scribes in 2026 ranking. For NP-specific tool selection, see our best AI scribe for medical professionals guide.
What to Look For in a Nursing AI Scribe
Nursing documentation is not physician documentation with different ratios. Before choosing a tool, evaluate it against these eight criteria:
1. ADPIE / DAR / FDAR Structure Support. The AI must produce nursing-format notes — ADPIE for full nursing process documentation, DAR or FDAR for focused notes — not SOAP. The format affects how the documentation reads to nursing leadership, surveyors, and other RNs taking handoff.
2. NANDA-I Nursing Diagnosis Recognition. The AI should recognize and structure NANDA-I 2024-2026 nursing diagnoses with code (e.g., Acute Pain 00132, Risk for Falls 00155, Impaired Skin Integrity 00046, Anxiety 00146, Ineffective Airway Clearance 00031, Risk for Infection 00004, Risk for Bleeding 00206, Decreased Cardiac Output 00029, Ineffective Tissue Perfusion 00204) with related-to (etiology) and as-evidenced-by (defining characteristics).
3. Risk Scale Capture Across Settings. Braden (pressure injury), Morse Falls Scale, Hendrich II Fall Risk Model, NEWS2 / MEWS, CIWA-Ar, CINA, Glasgow Coma Scale, RASS, CAM-ICU, BPS, CPOT, NRS, Wong-Baker FACES, FLACC, PAINAD. The AI should select the appropriate scale by patient population and capture the score into structured fields with trending.
4. SBAR and IPASS Handoff Generation. End-of-shift SBAR or IPASS document generation from the shift's accumulated documentation, with explicit Situation, Background, Assessment, Recommendation sections (or Illness severity, Patient summary, Action list, Situation awareness, Synthesis for IPASS).
5. Setting-Specific Templates. Med-surg q4h assessment, step-down q2h, ICU q1-2h hemodynamics with vasopressor titration, ED triage with ESI level, L&D delivery and post-partum, NICU q1-3h care, peds, oncology infusion documentation, hospice IDG and visit documentation, home health OASIS-E, school nurse daily log, occupational health post-incident.
6. Five (Eight) Rights Medication Administration. Structured documentation of right patient, right drug, right dose, right route, right time — with right documentation, right reason, right response added in many institutions. Exception documentation when a med is held, refused, or substituted.
7. SEP-1 and Bundle Compliance Templates. CMS SEP-1 sepsis bundle (lactate within 3 hours, blood cultures before antibiotics, broad-spectrum antibiotics within 1 hour, IV fluids 30 mL/kg for hypotension or lactate ≥4, vasopressors for persistent hypotension, lactate redraw within 6 hours if elevated). CAUTI/CLABSI/VAP/SSI bundle documentation. Pressure injury prevention bundle.
8. EHR Integration with Inpatient and Ambulatory. Bidirectional integration with Epic (Hyperdrive, Rover for nurse mobile), Cerner (Oracle Health), MEDITECH, Allscripts, athenahealth, eClinicalWorks. Hospital nursing has different EHR access patterns than ambulatory — mobile-friendly capture at bedside, integration with the eMAR, and write-back to flowsheets matter.
Detailed Reviews
1. DeepCura — Best Overall for Nursing Documentation
DeepCura is a customizable clinical AI platform that combines ambient scribing, clinical decision support, evidence search, practice automation, and bidirectional EHR integration — $129/month with unlimited notes. For nursing teams in ambulatory, hospital, home health, hospice, and school nurse settings — particularly those operating in independent practices, FQHCs, smaller hospitals, or as independent contractors — DeepCura's customizable templates and unlimited per-user notes deliver the strongest fit because no off-the-shelf scribe ships with NANDA-I/ADPIE/risk-scale structure out of the box.
For nurses, the key differentiator is template flexibility. DeepCura's custom template builder lets clinical informatics specialists encode nursing-specific templates: a med-surg q4h assessment template with focused systems review, NANDA-I diagnosis prompt, risk scale capture (Braden, Morse, NEWS2), pain reassessment, and intervention/response documentation; an ICU q1-2h template with continuous monitoring fields (HR, MAP, CVP, SpO2, EtCO2), vasopressor titration ladder, sedation (RASS) and analgesia (CPOT/BPS), ventilator settings, I&O hourly, and SEP-1 bundle compliance fields; an ED triage template with ESI-5 level, focused HPI, vitals trend, pain score, allergies, and disposition prep; a home health OASIS-E template with the 100+ M-codes; a school nurse daily log with medication administration, head injury check, and student visit reasons.
CDS Mode (3 credits per encounter) generates clinical decision support — particularly valuable for triage RNs handling phone consultations, RRT/MET (Rapid Response/Medical Emergency Team) responders structuring early-warning documentation, and care management RNs structuring TCM/CCM activities.
DeepEvidentia — DeepCura's evidence search engine — pulls from PubMed, AHRQ practice guides, AACN Practice Alerts, ANA/ANCC Magnet documentation requirements, Lippincott Procedures and Advisor references, and CMS SEP-1 specifications. Useful for bedside RNs verifying procedure steps, charge nurses checking policy alignment, and educators building competency-based documentation.
Strengths:
- Custom templates per setting (med-surg, ICU, step-down, ED, L&D, NICU, peds, oncology, hospice, home health, school, occ health) with ADPIE / DAR / FDAR structure
- NANDA-I 2024-2026 nursing diagnosis recognition with related-to and as-evidenced-by structuring
- Risk scale capture (Braden, Morse, Hendrich II, NEWS2/MEWS, CIWA-Ar, RASS, CAM-ICU, GCS, BPS/CPOT, NRS/FLACC/PAINAD)
- SBAR and IPASS handoff document generation from shift documentation
- SEP-1, CAUTI, CLABSI, VAP bundle templates
- AI receptionist for after-hours triage and intake — particularly valuable for telephone triage RNs and ambulatory nursing teams
- Multiple AI engines matched to documentation complexity (1-15 credits)
- Unlimited notes per provider on all plans
- Integration with Epic and Cerner via HL7/FHIR endpoints with custom field mapping; native integrations with athenahealth, AdvancedMD, and eClinicalWorks. DeepCura is not affiliated with Epic Systems Corporation or Oracle Health/Cerner.
Limitations:
- Custom template builder requires meaningful initial setup (15-25 hours for a multi-setting nursing department to encode templates per unit)
- Native Epic Rover and Cerner mobile-nurse integrations are via API/mapping rather than out-of-box mobile apps; ambient capture at bedside requires verifying device strategy
- Specialty nursing (NICU, oncology, hospice IDG) requires meaningful template engineering to match unit-specific conventions
Pricing: $129/month per provider — all features included. Free trial available, no credit card required.
Verdict: DeepCura is the strongest choice for nursing teams operating outside the largest enterprise health systems — independent practices, ambulatory specialty groups, smaller hospitals, FQHCs, home health agencies, hospice agencies, and school nursing programs. The flexibility cost is upfront setup time, but the per-user pricing and unlimited notes make it economically viable at small and mid-scale.
DeepCura: Customizable AI Scribe for Nursing
ADPIE / DAR / FDAR templates, NANDA-I diagnosis structure, Braden/Morse/NEWS2 risk capture, SBAR handoff generation, SEP-1 bundle support, and unlimited notes — $129/mo. Start your free trial.
+1 (415) 549-1829Available 24/7 · Set up in seconds · No credit card required
2. Abridge AI — Best for Hospital System Nursing
Abridge has emerged as the leading enterprise AI scribe for large health systems, with deployments at multiple major academic medical centers and integrated delivery networks. The product is sold via custom enterprise contracts and supports nursing workflows across inpatient, outpatient, and ED settings with deep Epic integration.
For hospital systems, Abridge offers consistent infrastructure for the full clinical team including nursing — RN documentation, charge nurse handoff, RRT/MET response, and care management. The product is well-tuned for the operational scale and compliance constraints of academic medical centers.
The limitation is access — Abridge is enterprise-only and not available to small hospitals, ambulatory practices, or independent nursing services. Pricing is custom (per-provider per-month with multi-year contracts).
Pricing: Custom enterprise contracts. Multi-year minimum.
Verdict: Best for hospital systems with enterprise procurement processes and Epic deep integration requirements. Read our Abridge AI review.
3. Nuance DAX Copilot — Best for Deep Epic / Cerner Nursing Integration
Nuance DAX Copilot (Microsoft) is the incumbent enterprise AI scribe with the extensive Epic and Cerner integration in the market. DAX Copilot supports nursing workflows in health-system contexts and integrates ambient documentation into Epic Hyperdrive, Epic Rover (nurse mobile), and Cerner workflows.
For health systems already on Microsoft enterprise contracts (M365, Azure, Teams), DAX Copilot is the path-of-least-procurement-resistance and offers consistent infrastructure across roles including bedside nursing.
The limitations parallel Abridge: enterprise-only, multi-year contracts, custom implementation. Not accessible to small independent practices or smaller hospitals.
Pricing: Custom enterprise. Multi-year contracts.
Verdict: Best for hospital systems on Microsoft enterprise contracts with Epic or Cerner.
4. Suki AI — Best Voice-First Nursing Tool
Suki AI offers a voice-first ambient and dictation product that some nursing leadership has adopted for ambulatory and selected inpatient workflows. The voice-first interaction model fits some nursing settings where ambient passive capture is impractical (NICU at-bedside with infant in incubator; ICU at-bedside with continuous monitoring noise; isolation rooms with PPE) but voice command is workable.
Suki's strengths are EHR integration depth (Epic, Cerner, athenahealth), the voice-first paradigm for active dictation, and a mature commercial deployment record.
Limitations for nursing-specific use: Suki's primary commercial focus is physician/APP rather than RN-specific templates, and NANDA-I/ADPIE/Braden-Morse structure is not natively pre-loaded.
Pricing: Approximately $199/month per user.
Verdict: Best for nursing settings where voice-first dictation is preferred over ambient capture and EHR integration depth matters more than nursing-specific template depth.
5. Heidi Health — Best Free Tier for RN Trial
Heidi Health offers a usable free tier (limited notes per month) that lets individual RNs test ambient AI documentation at zero cost. Heidi has multi-role templates available across specialties and adapts to nursing workflows with custom configuration. International product traction in Australia, NZ, and the UK is stronger than US — and notably, Australian and UK nursing documentation conventions (NMC standards, ANMC standards) are reasonably well-supported.
EHR integration is limited (clipboard or email), and US nursing conventions (Joint Commission, CMS SEP-1, US-specific risk scales) require some custom configuration.
Pricing: Free tier (limited notes), Pro tier roughly $99/month, enterprise tier higher.
Verdict: Best for individual RNs and small nursing services who want to test ambient AI documentation at zero cost before committing to a paid tool. Read our Heidi Health review.
6. Freed AI — Best for Nurse Practitioners
Freed AI is the most accessible option for nurse practitioners working in primary care, urgent care, and outpatient specialty practice — but Freed is built around the APP/physician encounter model rather than RN-specific documentation. NPs running independent practices where they bill 99202-99215 E&M visits will find Freed efficient for their physician-style note workflow; bedside RNs in inpatient settings will find Freed less applicable.
Pricing: $39/month (Starter, 40 notes), $79/month (Core, unlimited), $104/month (Premier, unlimited + EHR push + ICD-10).
Verdict: Best for NPs with primary care or specialty E&M practice workflows. Not the right fit for bedside RNs in inpatient or skilled nursing settings. Read our Freed AI review.
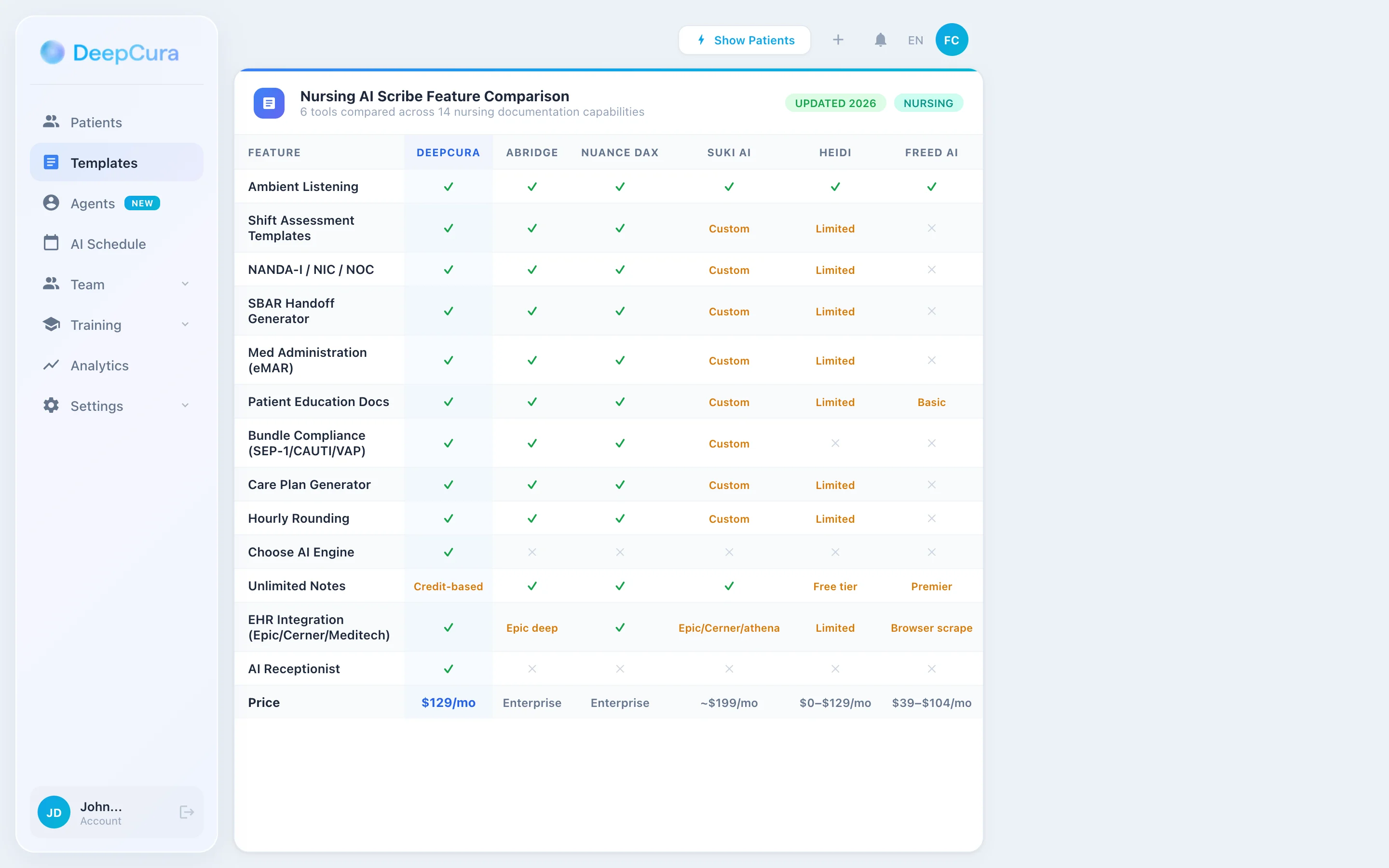
Head-to-Head — Nursing Documentation Features
| Feature | DeepCura | Abridge | Nuance DAX | Suki | Heidi | Freed |
|---|---|---|---|---|---|---|
| ADPIE / DAR / FDAR Structure | ✓ Custom | ✓ Enterprise | ✓ Enterprise | Custom | Limited | ✗ |
| NANDA-I Diagnosis Recognition | ✓ | ✓ Enterprise | ✓ Enterprise | Custom | Limited | ✗ |
| Risk Scale Capture (Braden/Morse/NEWS2/CIWA) | ✓ | ✓ | ✓ | Custom | Limited | ✗ |
| SBAR / IPASS Handoff | ✓ | ✓ | ✓ | Custom | Limited | ✗ |
| Pain Scales (NRS/FLACC/PAINAD/CPOT/BPS) | ✓ | ✓ | ✓ | Custom | Limited | ✗ |
| Med-Surg q4h Template | ✓ Custom | ✓ Enterprise | ✓ Enterprise | Custom | Limited | ✗ |
| ICU q1-2h Template | ✓ Custom | ✓ Enterprise | ✓ Enterprise | Custom | Limited | ✗ |
| ED Triage with ESI Level | ✓ Custom | ✓ Enterprise | ✓ Enterprise | Custom | Limited | ✗ |
| Home Health OASIS-E | ✓ Custom | Custom | Custom | ✗ | ✗ | ✗ |
| 5/8 Rights Med Admin | ✓ | ✓ | ✓ | Custom | Limited | ✗ |
| SEP-1 Bundle Template | ✓ | ✓ | ✓ | Custom | ✗ | ✗ |
| AI Receptionist (telephone triage) | ✓ | ✗ | ✗ | ✗ | ✗ | ✗ |
| Clinical Decision Support | ✓ (CDS Mode) | Limited | ✗ | ✗ | ✗ | ✗ |
| EHR Bidirectional | 9 EHRs | Epic deep | Epic/Cerner deep | Epic/Cerner/athena | Limited | Browser scrape |
| Price | $129/mo all features | Enterprise custom | Enterprise custom | ~$199/mo | $0-$99/mo | $39-$104/mo |
Nursing Workflow with DeepCura
DeepCura's tiered credit system lets nursing teams match AI resources to documentation complexity — fast for routine assessments, deeper for transitions and complex care.
Routine Shift Assessment (1 Credit) — q4h Med-Surg, q2h Step-Down
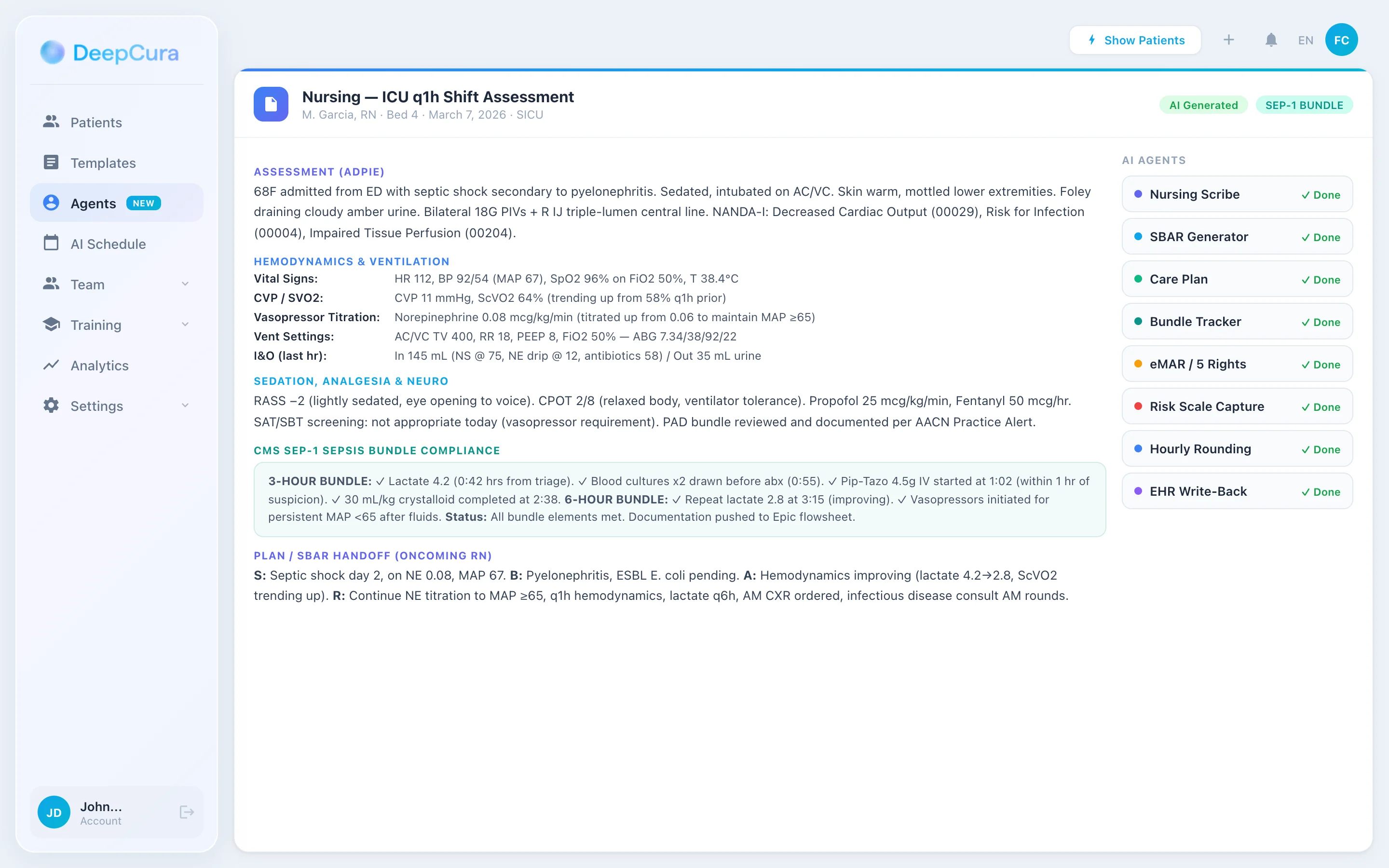
For routine interval assessments — q4h med-surg with focused systems review, vital trend, pain reassessment, intervention documentation; q2h step-down with hemodynamics, ongoing IV therapy, and patient response — the 1-credit model generates a complete ADPIE or DAR-format note in under 30 seconds. Speed-optimized for the high-volume shift where an RN with a 5-patient assignment needs documentation completion to maintain the bedside-to-charting ratio.
Complex Documentation (3 Credits CDS) — Admission, Transfer, Discharge
For high-volume documentation events — initial admission assessment with complete head-to-toe, baseline risk scales, code status review, HPI integration, and care plan initialization; transfer of care with SBAR handoff document generation; discharge with teaching documentation, teach-back validation, and follow-up coordination — CDS Mode generates clinical decision support and structures the multi-section narrative across the patient's continuum.
Critical Care, RRT, and Code Documentation (15 Credits) — ICU Hemodynamics, RRT/MET Response, Code Documentation
For ICU q1-2h continuous documentation with vasopressor titration, sedation/analgesia ladder, ventilator changes, and ongoing assessment; rapid response team activations with timeline accuracy required; resuscitation events requiring time-stamp accuracy for code review — the maximum-depth model produces complete narratives with continuous timeline integration, intervention attribution to team members, and post-event SBAR/IPASS for handoff.
From Bedside to Documentation in Real Time
DeepCura templates for med-surg, ICU, ED, L&D, home health, and school nursing with NANDA-I, ADPIE, risk scales, SBAR, and SEP-1 bundle support — built for the nursing workflow. Start your free trial.
+1 (415) 549-1829Available 24/7 · Set up in seconds · No credit card required
Clinical Decision Support and Evidence Search for Nurses
CDS Mode outputs are documentation-aid suggestions for clinician review. They are not diagnoses, treatment recommendations, or substitutes for clinical judgment. The clinician retains full responsibility for assessment, escalation, and intervention decisions within their scope of practice. DeepCura is not an FDA-cleared medical device.
CDS Mode — Decision Support at the Bedside and on the Phone
Telephone triage RNs, charge nurses, RRT/MET responders, and care management RNs benefit directly from clinical decision support. A telephone triage RN handling a parent calling about a 3-year-old with fever and cough needs structured triage decision logic (Schmitt-Thompson protocols, Briggs Pediatric Telephone Triage). A charge nurse weighing whether to call RRT for a patient with deteriorating vitals needs early-warning calibration (NEWS2 trend, MEWS, qSOFA). CDS Mode provides differential considerations and triage guidance calibrated to the clinical scenario.
For an RN encountering a med-surg patient with new tachycardia, hypotension, and decreased urine output, CDS Mode flags: hypovolemia (most likely; rule-out blood loss, GI losses, third-spacing), early sepsis (NEWS2 trending up; consider blood cultures, lactate, broad-spectrum antibiotics if clinical suspicion meets SEP-1 trigger), cardiogenic shock (consider in cardiac history), and adverse medication effect (review recent medication administration). The differential supports both the documented clinical reasoning and the timely escalation to provider.
DeepEvidentia — Evidence at the Bedside for Nurses
DeepEvidentia provides real-time access to PubMed, AHRQ practice guides, AACN Practice Alerts, ANA Standards of Practice, Lippincott Procedures and Advisor (where licensed), CMS SEP-1 specifications, NDNQI nursing-sensitive indicators, AHRQ TeamSTEPPS resources, and policy library references.
Example queries nurses actually ask:
- "SEP-1 bundle compliance — lactate redraw timing requirement" — returns CMS SEP-1 specifications with 6-hour redraw rule for elevated initial lactate
- "Braden Scale cutoff for pressure injury prevention bundle initiation" — returns AHRQ guidelines with ≤18 high risk threshold and bundle activation
- "NEWS2 score thresholds for MET activation" — returns Royal College of Physicians NEWS2 scoring with ≥7 immediate clinical review trigger
- "CIWA-Ar scoring intervals and pharmacologic protocols" — returns Sullivan et al. CIWA-Ar reference and ASAM withdrawal management guidelines
- "CDC Hand Hygiene Guidelines — alcohol-based hand rub vs soap and water indications" — returns 2002 CDC Guideline (still current) with C. difficile soap and water indication
- "AACN Practice Alert on alarm management" — returns the alarm fatigue prevention bundle
For clinical informatics specialists building competency programs, charge nurses verifying policy in real-time, and bedside RNs encountering an unfamiliar protocol, evidence access at the bedside meaningfully reduces the friction of staying current.
Pricing Comparison
| Tool | Monthly | Note Limit | Nursing-Specific | Best Plan |
|---|---|---|---|---|
| DeepCura | $129/mo | Unlimited | ✓ Custom NANDA/ADPIE | Single plan, all features |
| Abridge AI | Enterprise custom | Enterprise | ✓ | Enterprise contract |
| Nuance DAX Copilot | Enterprise custom | Enterprise | ✓ | Enterprise contract |
| Suki AI | ~$199/mo | Unlimited | Voice-first | Pro tier |
| Heidi Health | $0-$99/mo | Free tier limited | Limited | Free or Pro |
| Freed AI | $39-$104/mo | 40-unlimited | NP-only | Premier ($104) — for NPs |
See DeepCura in Action
Watch how DeepCura handles the full nursing workflow — ADPIE/DAR/FDAR notes, NANDA-I diagnosis structure, risk scale capture (Braden, Morse, NEWS2, CIWA-Ar), SBAR/IPASS handoff generation, SEP-1 bundle compliance, evidence search via DeepEvidentia, and AI receptionist for telephone triage.

Frequently Asked Questions
What is the best AI scribe for nurses?
DeepCura is the strongest cross-functional choice for nursing teams operating outside the largest enterprise health systems — independent practices, ambulatory specialty groups, smaller hospitals, FQHCs, home health agencies, hospice agencies, and school nursing programs. Customizable templates support ADPIE/DAR/FDAR, NANDA-I diagnoses, risk scales, SBAR handoff, and SEP-1 bundle workflows. For large hospital systems with Epic deep integration requirements, Abridge AI and Nuance DAX Copilot are the enterprise leaders.
Do AI scribes support NANDA-I nursing diagnoses and ADPIE structure?
DeepCura supports custom NANDA-I 2024-2026 nursing diagnosis recognition with related-to (etiology) and as-evidenced-by (defining characteristics) structure, and ADPIE / DAR / FDAR note formats. Enterprise tools (Abridge, Nuance DAX Copilot) support nursing-specific structures in their workflows. Solo-focused tools (Freed) and free-tier tools (Heidi) do not have native NANDA-I support — practices using these tools manually map nursing language.
Can AI scribes capture Braden, Morse, NEWS2, CIWA-Ar, and other risk scales?
DeepCura supports structured capture of Braden Scale, Morse Falls Scale, Hendrich II Fall Risk, NEWS2/MEWS, CIWA-Ar, CINA, Glasgow Coma Scale, RASS, CAM-ICU, BPS, CPOT, NRS, Wong-Baker FACES, FLACC, PAINAD with population-appropriate scale selection and trending. Enterprise tools support these scales in their respective workflows.
Do AI scribes generate SBAR and IPASS handoff documents?
DeepCura generates SBAR (Situation, Background, Assessment, Recommendation) and IPASS (Illness severity, Patient summary, Action list, Situation awareness, Synthesis) handoff documents from accumulated shift documentation. Enterprise tools support handoff generation in their workflows. Solo and free-tier tools do not have native SBAR/IPASS handoff generation.
Can AI scribes support CMS SEP-1 sepsis bundle and CAUTI/CLABSI prevention bundle documentation?
DeepCura's templates can be configured for CMS SEP-1 (lactate within 3 hours, blood cultures before antibiotics, antibiotics within 1 hour, fluids 30 mL/kg, vasopressors for persistent hypotension, lactate redraw within 6 hours), CAUTI prevention bundle, CLABSI prevention bundle, VAP prevention bundle, and SSI prevention bundle. Enterprise tools support bundle documentation. Solo and free-tier tools require manual bundle documentation.
Do AI scribes integrate with Epic Hyperdrive / Rover, Cerner, and MEDITECH for inpatient nursing?
DeepCura integrates with Epic, Cerner, and other major hospital EHRs via bidirectional API integration with custom field mapping. Abridge has the extensive Epic Hyperdrive integration in the enterprise market. Nuance DAX Copilot has deep Epic and Cerner integration. Suki AI integrates with Epic, Cerner, and athenahealth. MEDITECH integration is more limited across the AI scribe market — practices on MEDITECH should verify integration depth during evaluation.
Are AI scribes appropriate for home health OASIS-E documentation?
DeepCura's templates can be configured for home health OASIS-E (the 100+ M-codes in the Outcome and Assessment Information Set, version E). Most enterprise and solo AI scribes do not have native OASIS-E support. Home health agencies should verify OASIS-E template depth during evaluation since OASIS errors directly affect HH-PPS payment and quality reporting.
How much do AI scribes for nurses cost?
Solo-friendly options run $39-$130/month per user (Freed $39-$104, Heidi Pro $99, DeepCura $129). Suki is approximately $199/month per user. Enterprise tools (Abridge, Nuance DAX Copilot) are custom-priced with multi-year contracts. For most nursing teams operating outside the largest hospital systems, the $99-$150/month accessible-price tier offers the best feature-to-cost ratio with DeepCura providing the extensive nursing-specific template support at that price point.
Final Verdict
For nursing teams, the choice comes down to four profiles:
Best overall: DeepCura at $129/month — customizable ADPIE/DAR/FDAR templates, NANDA-I 2024-2026 nursing diagnoses, risk scale capture (Braden, Morse, NEWS2, CIWA-Ar, GCS, RASS, CAM-ICU, BPS, CPOT, NRS, FLACC, PAINAD), SBAR and IPASS handoff generation, SEP-1 and prevention bundle templates, AI receptionist for telephone triage, and unlimited notes per provider. The strongest choice for nursing teams operating outside the largest enterprise health systems.
Best for hospital systems: Abridge AI and Nuance DAX Copilot — enterprise-grade with deep Epic and Cerner integration, multi-role/multi-setting deployment, and the IT/security/legal frameworks that academic medical centers and large IDN organizations require. Custom enterprise pricing.
Best for voice-first nursing: Suki AI at approximately $199/month — voice-first ambient and dictation with deep Epic, Cerner, and athenahealth integration. Best for nursing settings where ambient passive capture is impractical (NICU, ICU at-bedside, isolation rooms with PPE) but voice command is workable.
Best for free-tier RN trial: Heidi Health — free tier (limited notes) lets individual RNs and small nursing services test ambient AI documentation at zero cost.
For a broader cross-specialty comparison, see our Best AI Medical Scribes in 2026 ranking. For NP-specific tool selection, see our best AI scribe for medical professionals and best AI scribe for physicians guides. For practices needing after-hours triage automation, see our Best AI Medical Receptionist guide. For free copy-paste clinical templates, see our SOAP note template reference. If you are evaluating EMRs alongside the scribe decision, see our best EMR for small practices ranking.
References
[1] National Council of State Boards of Nursing, "2024 Nurse Workforce Study," NCSBN. ncsbn.org/research/recent-research
[2] American Nurses Association, "Nursing: Scope and Standards of Practice, Fourth Edition," ANA. nursingworld.org/practice-policy/scope-of-practice
[3] NANDA International, "NANDA-I Nursing Diagnoses: Definitions and Classification 2024-2026, Thirteenth Edition," NANDA-I. nanda.org
[4] Royal College of Physicians, "National Early Warning Score (NEWS) 2 — Standardising the assessment of acute-illness severity in the NHS," RCP. rcp.ac.uk/improving-care/resources/national-early-warning-score-news-2
[5] Bergstrom N, Braden B, Laguzza A, Holman V, "The Braden Scale for Predicting Pressure Sore Risk," Nursing Research, 36(4), 205-210, 1987. bradenscale.com
[6] Morse JM, Black C, Oberle K, Donahue P, "A prospective study to identify the fall-prone patient," Social Science & Medicine, 28(1), 81-86, 1989. AHRQ summary: ahrq.gov/patient-safety/settings/long-term-care
[7] Sullivan JT, Sykora K, Schneiderman J, Naranjo CA, Sellers EM, "Assessment of Alcohol Withdrawal: The Revised Clinical Institute Withdrawal Assessment for Alcohol Scale (CIWA-Ar)," British Journal of Addiction, 84(11), 1353-1357, 1989. pubmed.ncbi.nlm.nih.gov/2597811
[8] Centers for Medicare & Medicaid Services, "Hospital Inpatient Quality Reporting (IQR) Program — SEP-1 Severe Sepsis and Septic Shock Bundle," CMS QualityNet. qualitynet.cms.gov/inpatient/iqr
[9] American Association of Critical-Care Nurses, "AACN Practice Alerts," AACN. aacn.org/clinical-resources/practice-alerts
[10] The Joint Commission, "Hospital Accreditation Standards — Record of Care, Treatment, and Services (RC) Standards," TJC. jointcommission.org
[11] Agency for Healthcare Research and Quality, "TeamSTEPPS — Evidence-Based Teamwork System (SBAR, IPASS, Handoffs)," AHRQ. ahrq.gov/teamstepps